

Unpopular Opinion: AI Scribes Are Hiding a Bigger Problem
Ambient AI tools are delivering real but limited burnout relief - while health systems use them as cover to avoid the harder conversation about what actually makes physicians quit.


Here is what $1.6 billion in AI investment bought the American healthcare system in 2025: a tool that listens to physician conversations and writes the note for them.
The early data is genuinely good. A study of 263 physicians across six health systems found burnout dropped from 51.9% to 38.8% after 30 days with an ambient AI scribe. Documentation time fell by more than 15%. Physicians report feeling less trapped by their keyboards. That is real. That matters.
But here is what the press releases do not say: 62% of physicians still reported burnout in 2025 according to Medscape. The 13-point improvement is meaningful, but it is happening against a baseline so broken that two-thirds of the physician workforce is still experiencing clinical exhaustion even with the tools in place.
The ambient AI scribe is a good answer to a symptom. Health systems are treating it as a cure for a disease it does not touch.

1. The Ambient AI Boom Is Real - and Genuinely Promising
Let us be precise about what ambient AI scribes actually accomplish, because the technology is not the problem.
The tools - Abridge, Nuance DAX, Freed AI, and Epic's native "Art for Clinicians" - listen passively to physician-patient conversations and generate structured clinical notes. No dictation. No keyboard. The physician reviews and signs. Visit time shifts from note-typing back to the patient in front of them.
The adoption curve is steep. By 2025, 62.6% of Epic hospitals were live with generative AI tools, and 71% of physician practice leaders reported using AI for patient visits. Investors poured $1.6 billion into ambient AI companies in 2025 alone. Abridge raised $550 million across two rounds and achieved a $5.3 billion valuation. Epic built its own competing tool. Nuance - already inside Microsoft - accelerated deployment.
The market is not hype. The clinical evidence is emerging and it is directionally positive.
📊 A 2025 randomized study found ambient AI users spent 8.5% less total time in the EHR and 15% less time composing notes specifically.
The problem is not the technology. The problem is the narrative layered on top of it.

2. What the Data Shows - and What It Quietly Omits
Every ambient AI study shows improvement on documentation metrics. The burnout studies show partial improvement. Both are real. Neither tells the whole story.
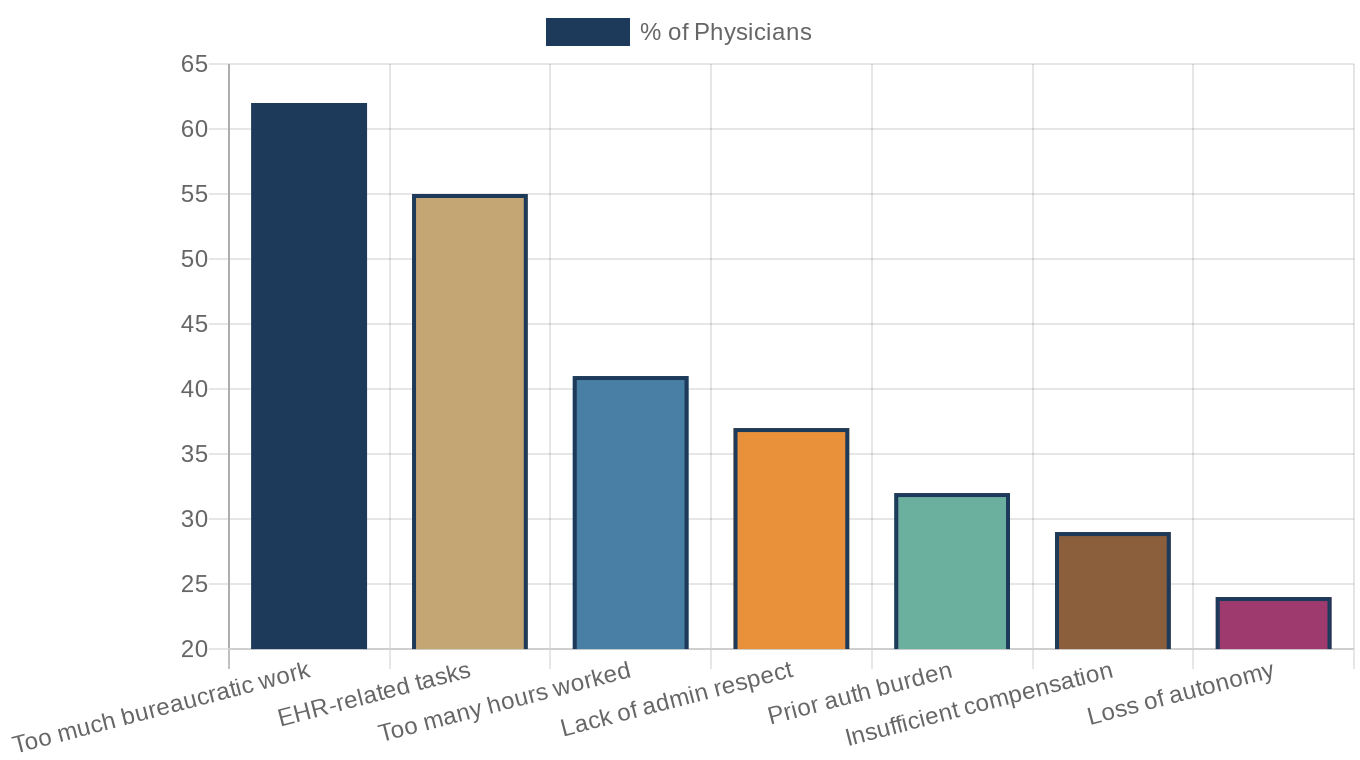
When Medscape surveyed physicians in 2025 and asked them to name their top burnout drivers, "too much bureaucratic work" came in first at 62%. "EHR-related tasks" came second at 55%. Those two dominate the rankings and they are the exact things ambient AI addresses.
But look further down the list. "Too many hours worked" at 41%. "Lack of respect from administrators" at 37%. "Prior authorization burden" at 32%. "Loss of autonomy" at 24%.
These are structural causes. They predate EHRs. They will not respond to a better microphone in the exam room.
The chart below shows how physician burnout drivers stack up - and which ones ambient AI actually addresses:
A physician who spends less time on notes is still receiving 77 EHR inbox messages per day - a figure documented in a 2025 multi-site study. They are still completing 43 prior authorizations every week, burning more than 16 hours on forms, hold music, and appeals that have nothing to do with patient care. They are still working within a 15-minute visit slot that RVU production targets have compressed over decades.
The ambient AI scribe does not touch any of those problems. And the studies that show burnout reduction from AI scribes are, almost by design, measuring the thing the tool addresses while leaving the rest of the iceberg unmeasured.

3. The RVU Trap That AI Cannot Fix
To understand why AI scribes are insufficient, you need to understand what actually compressed physician time in the first place.
The Relative Value Unit system - how Medicare and most payers compensate physicians - assigns point values to clinical activities. A basic 15-minute office visit (CPT code 99213) carries approximately 1.30 wRVUs. A complex 45-minute visit (99215) carries 2.80 wRVUs. The math heavily incentivizes volume: more shorter visits generate more wRVUs than fewer longer ones.
Health systems, facing relentless margin pressure, set productivity targets based on these benchmarks. The 2026 MGMA benchmark for Family Medicine sits at 5,033 median wRVUs per year. Primary care physicians are effectively scheduled to produce that number - which means scheduling templates designed to maximize E&M visit throughput, defaulting to 15-minute slots.
📊 From 2023 to 2024, median total encounters rose 7.81% for primary care physicians even as median wRVUs fell - meaning they are seeing more patients for less compensation per encounter, while clinical complexity continues to rise.
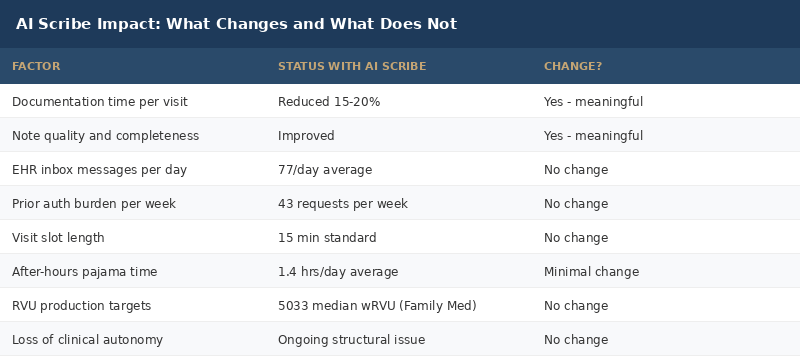
The ambient AI scribe does not change this math. A physician who uses an AI scribe can write the note faster. The note is cleaner. The review takes less time. But the 15-minute slot is still 15 minutes. The next patient is still waiting. The RVU target is still 5,033. The production pressure is structural. The tool is cosmetic.
If a health system implements ambient AI and then uses the recovered time to squeeze one more patient visit into the schedule, the tool has not reduced burnout. It has enabled a new layer of throughput pressure.
This is not hypothetical. It is the predictable consequence of deploying efficiency tools into an incentive structure that absorbs every efficiency gain and converts it into more volume.
The table below shows precisely where AI scribes move the needle - and where they do not:
4. The 77-Message Inbox That Ambient AI Ignores
There is a specific physician workflow failure that almost never makes it into the ambient AI marketing materials: the EHR inbox.
Physicians receive an average of 77 EHR inbox messages per day. These are not spam. They are patient portal messages, lab results requiring review and action, refill requests, administrative flags, specialist notes, and care coordination tasks. Each one requires physician judgment. None of them can be delegated to an AI scribe that listens to exam room conversations.
Primary care physicians average 2.7 hours of after-hours EHR work daily - uncompensated time done after clinic ends. This is the inbox catching up to them after a full day of patient visits. It is a second shift performed for free, invisible in RVU calculations and scheduling templates.
Ambient AI scribes have zero impact on this. The tool records the encounter. The note writes itself. The physician goes home - and opens the inbox.
📊 Clinicians using ambient AI tools spend 8.5% less total time in the EHR per encounter, but the inbox burden runs on its own unmanaged cycle entirely separate from documentation.
The solutions to inbox overload are not AI scribes. They are staff-supported inbox triage - having MAs or nurses handle refills, stable lab review, and routing before it reaches the physician - team-based care models, visit preparation protocols that front-load information collection, and EHR design that reduces inbox generation in the first place. These require staffing investment and organizational redesign. Not a new software subscription.

5. Prior Authorization: The 16-Hour-a-Week Tax
If inbox overload is the quiet burnout driver nobody talks about, prior authorization is the loud one nobody fixes.
Physicians complete an average of 43 prior authorizations per week, dedicating more than 16 hours to the process - forms, phone calls, hold queues, peer-to-peer reviews, and denials that must be appealed. This is equivalent to 40% of a physician's working week consumed by an administrative process designed to reduce payer cost by delaying or denying care.
26% of physicians reported that prior authorization delays directly harmed their patients in a 2025 AMA survey. The harms include cancer diagnoses delayed, imaging not performed, medications not started.
AI is making inroads here. AI-generated prior authorization letters show strong clinical content. CMS's CMS-0057-F rule required payers to build real-time API connections by January 2026, reducing some information asymmetry. Companies like Waystar, Infinitus, and Cohere Health are deploying AI against the prior authorization workflow.
But ambient AI scribes - the category receiving $1.6 billion in investment and generating the burnout headlines - do not address prior authorization. They listen to patient encounters. They do not negotiate with UnitedHealth.
📊 Physicians spend more than 16 hours per week on prior authorization - the equivalent of a full-time administrative role layered on top of clinical practice.
The prior authorization crisis is a policy problem masquerading as a workflow problem. The only real solutions are legislative limits on PA requirements, automatic approval for high-evidence standard-of-care treatments, and payer-side AI that can process requests in minutes rather than days. Health systems cannot solve this with a subscription to Abridge.
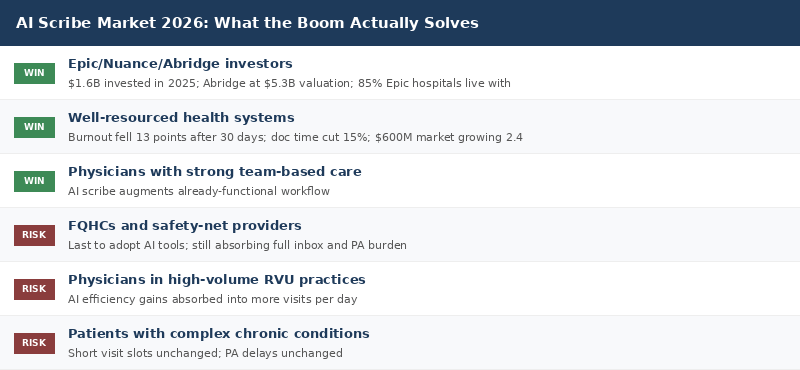
Below is a scorecard of who the current AI scribe boom is actually helping:
Deep Dive: The Financial Case for Full Workflow Redesign
The health systems actually reducing burnout - not just documentation time - share a common pattern. They are not just deploying AI scribes. They are using AI as the first step in a broader workflow redesign that addresses all five burnout drivers simultaneously.
What Comprehensive Redesign Includes
Step 1: AI Scribes (Documentation Layer)
Deploy ambient documentation. Recover 45 to 60 minutes per physician per day. Use this recovery to establish the organizational case for further change - not to add more visits.
Step 2: Inbox Triage Infrastructure (Staffing Layer)
Staff inbox triage teams of MAs or licensed staff per physician panel. Standardize refill protocols that do not require physician review. Route stable lab results to a patient notification workflow. Target: reduce physician inbox volume from 77/day to 30/day.
Step 3: Pre-Visit Preparation (Scheduling Layer)
30 minutes before each visit, a care coordinator reviews the chart, flags open orders, closes care gaps, updates medication lists, and queues priority issues. The physician walks in prepared. The 15-minute slot becomes productive instead of frantic.
Step 4: Prior Authorization Automation (Revenue Cycle Layer)
Deploy AI-powered PA tools to auto-submit standard-of-care requests with clinical documentation packages. Target: reduce PA hours from 16+ per week to 6 per week per physician.
Step 5: Schedule Redesign (Throughput Model Layer)
Extend complex visit slots. Reserve buffer time for urgent add-ons. Build explicit team huddle time into the daily schedule. This requires leadership authorization to reduce raw RVU production targets - which requires the financial model to show equivalent or higher margin from reduced turnover costs.
The financial argument is compelling. The chart below shows the math:
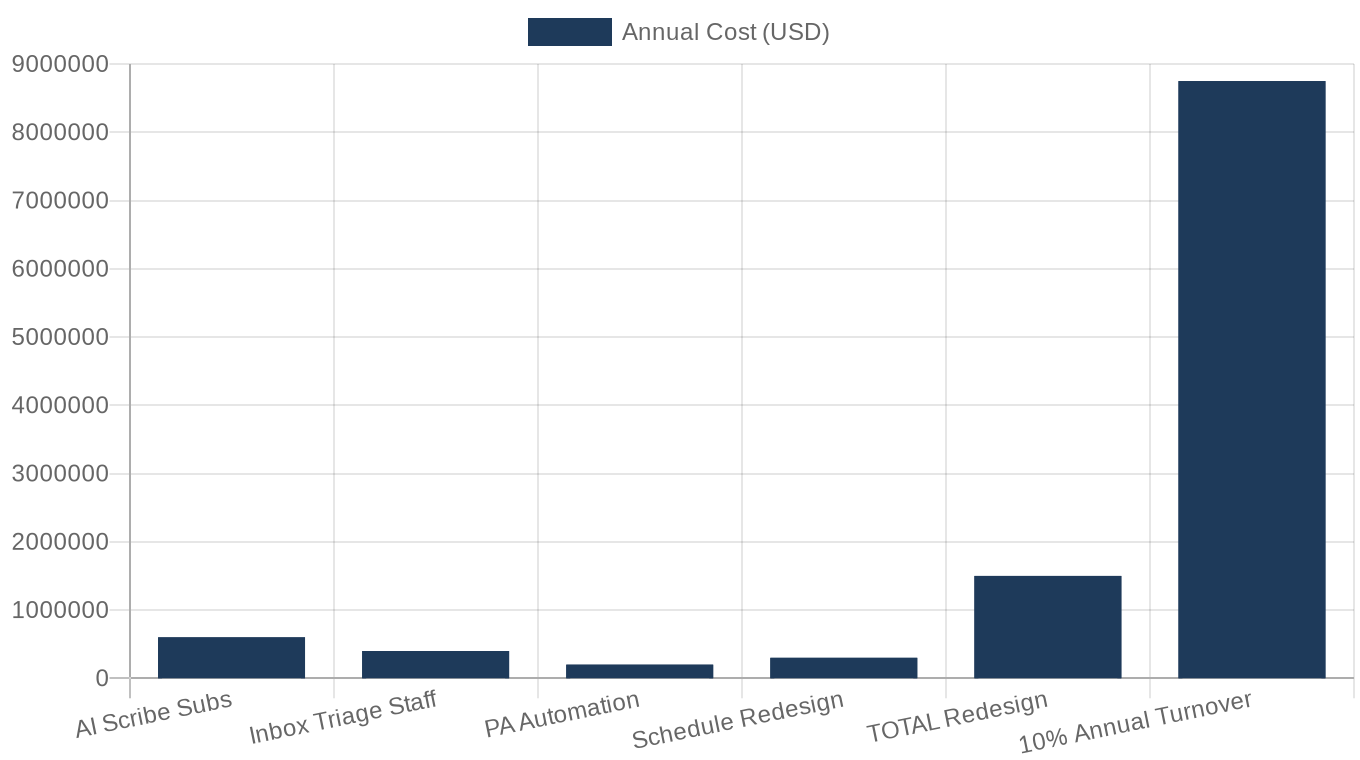
The average cost to replace a physician is $750,000 to $1 million when recruitment, onboarding, and locum coverage are factored in. A health system losing 10% of its physician workforce annually to burnout is spending $7.5M to $10M per 100 physicians in replacement cost alone. Full workflow redesign for a 100-physician practice - AI scribes, inbox triage staff, scheduling changes - costs approximately $1.5M to $2M annually. The ROI is not close.
The ambient AI scribe is the cheapest line in the redesign budget. It is also the most visible. Health systems are stopping there because the other steps are harder. They require staffing investment, scheduling authority changes, and a willingness to reduce short-term throughput in exchange for long-term physician retention.

What This Means For You
FQHC executives and community health center leaders: Ambient AI scribes are arriving at your doorstep as a burnout solution. They will help - but you are also facing the highest documentation burden, the thinnest staffing ratios, and the least access to inbox triage resources. Do not implement an AI scribe and call burnout solved. Budget for the staffing infrastructure that makes the tool effective: at least one MA per 1.5 physicians for inbox support and pre-visit prep.
Health system administrators and CMOs: You have deployed the AI scribe. Now do the harder work. Run a physician time audit across your top five burnout drivers - documentation, inbox, prior auth, visit slots, and administrative intrusions on clinical autonomy. AI scribes only close the first gap. Build the roadmap for all five.
Radiologists and pulmonologists: Your burnout drivers differ from primary care but the pattern is the same. AI tools are arriving to reduce reading time and report generation burden. Ask your department leadership what is being done about prior authorization delays for CT and MRI, about the overnight call coverage model, and about reading volume targets. Those are the conversations that matter.
Healthcare investors and founders: The ambient AI scribe market is not finished - but the next phase is integration, not documentation. The companies that win in 2027 are not building better microphones. They are building integrated workflow platforms that connect ambient documentation to inbox triage to PA automation to scheduling optimization. Single-feature AI tools are table stakes.
Policy advocates: Prior authorization is a federal policy problem. CMS-0057-F is a start, but automatic approval for standard-of-care treatments and real-time PA processing requirements for high-acuity conditions need to be in the next reauthorization package. Physician burnout at this scale is a public health crisis. The solution cannot be a better voice recorder.
Closing
The ambient AI scribe is not a distraction. It is a genuine tool delivering genuine value. A 13-point reduction in burnout among users is not nothing - in a workforce where 62% are burned out, that is tens of thousands of physicians who feel meaningfully better about their workday.
But American health systems have a habit of adopting the visible technology solution and declaring the underlying problem solved. We did it with EHRs in 2010. We told ourselves that digitizing records would transform care coordination. Fifteen years later, those same EHRs are the second-leading cause of physician burnout.
The ambient AI scribe is the right first step. Health system leaders need to say out loud that it is only the first step - and then fund the rest of the plan.
The physicians who are quietly updating their LinkedIn profiles right now are not leaving because they hate taking notes. They are leaving because the system surrounding the note-taking has not been redesigned in twenty years.
What would it take for your health system to actually fix the machine - not just tune it?
Reply and tell me. I read every response.
About the Author
Jonathan Govette is the Co-Founder and CEO of Oatmeal Health, an AI lung cancer diagnostic company catching cancers earlier in the communities that need it most. Oatmeal uses AI to identify unscreened high-risk patients, navigate them to care, and score every lung CT for malignancy risk - billed under CPT 0721T. Stage I survival is 77%. Stage IV is 9%. We work in FQHCs because that gap is largest there.
Jonathan writes daily about radiology, pulmonology, AI diagnostics, health policy, hospital operations, and healthcare startups.
Subscribe to stay ahead of healthcare's most important shifts.
Weekly deep-dives on AI, radiology, health policy, FQHCs, and the business of healthcare - written for operators, clinicians, and investors who want the signal, not the noise.
Subscribe at oatmealhealthjonathangovette.substack.com
Key References
Multi-site ambient AI scribe study (263 physicians, 6 health systems, Abridge/PMC 2025): burnout reduction from 51.9% to 38.8% after 30 days
Medscape Physician Burnout and Depression Report 2025: 62% of physicians reporting burnout, top-driver survey data
2025 multi-site study: physicians average 77 EHR inbox messages per day, 2.7 hours daily after-hours EHR work
AMA Prior Authorization Physician Survey 2025: 43 PA requests per week, 16+ hours consumed, 26% reporting patient harm
PitchBook/FierceHealthcare: $1.6 billion invested in ambient AI companies in 2025; Abridge $550M raised at $5.3B valuation
MGMA 2026 Benchmarks: Family Medicine median 5,033 wRVU; primary care encounter and productivity trends 2023-2024