

One Big Beautiful Bill: The FQHC Reckoning
Eleven million Americans are losing Medicaid under H.R.1, and FQHCs face a $7 billion annual uncompensated care surge with no revenue offset.


The bill was signed on July 4, 2025. Call it the One Big Beautiful Bill Act - OBBBA, H.R.1, whatever your preference. The name does not matter. The math does.
Between 9.9 and 14.9 million Americans are projected to lose health insurance under this law. The American Medical Association puts the figure at 11.8 million. The Congressional Budget Office, evaluating the House version, scored 5.2 million fewer insured adults by 2034 from work requirements alone - with 4.8 million losing coverage entirely.
Every one of those patients does not disappear. They get sick. They show up at community health centers. And the 1,400 FQHC organizations running nearly 15,000 sites across the country are legally required - as a condition of their federal funding - to see them, regardless of ability to pay.
That is not a policy nuance. That is the entire crisis in one sentence.
1. What the Law Actually Does, Provision by Provision
The headline number is $911 billion in Medicaid cuts over a decade. That is the figure that circulates in congressional briefings and policy newsletters. But for FQHC directors and community health center administrators, the story is not in the aggregate total. It is in the specific mechanisms and their implementation timelines - and how they stack.
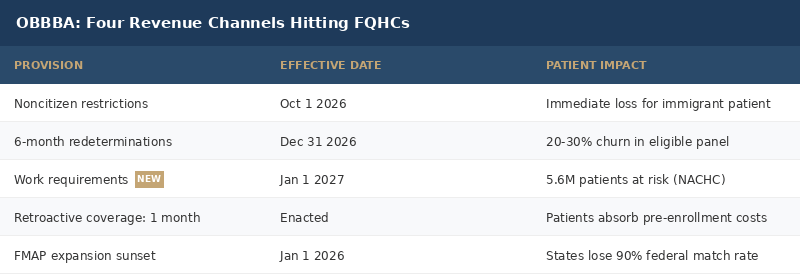
The OBBBA does not hit FQHCs through a single cut. It hits through four separate channels, on four separate timelines, each compounding the others.
Channel 1: Noncitizen Medicaid restrictions - effective October 1, 2026. The law significantly narrows Medicaid eligibility for noncitizens, removing coverage for many lawfully present immigrants who previously qualified. FQHCs in border states, major metros, and agricultural regions will feel this immediately. For some sites, noncitizen patients make up 20 to 40 percent of their patient panel.
Channel 2: Six-month Medicaid redeterminations - effective December 31, 2026. States must now conduct Medicaid eligibility reviews at least every six months - twice as often as before. Every six months, eligible patients must re-prove their eligibility. Experience from pre-2020 redeterminations shows that 20 to 30 percent of technically eligible patients lose coverage temporarily due to paperwork failures. Not because they are ineligible - because they could not navigate the portal or complete the documentation in time.
Channel 3: Retroactive coverage shortened to one month. Previously, Medicaid expansion enrollees could receive up to two months of retroactive coverage for care received before their application was processed. Under OBBBA, that window is now one month. When a patient presents for care before enrolling in Medicaid, the visit that prompted their enrollment is now less likely to be covered. The bill falls on the patient or the FQHC.
Channel 4: Work requirements - effective January 1, 2027. Adults ages 19 to 64 in the Medicaid expansion population must demonstrate 80 hours per month of qualifying community engagement - work, training, education, caregiving, or community service - or obtain a recognized exemption to maintain eligibility.
NACHC estimates 5.6 million community health center patients are at risk from work requirements alone. The CBO puts the broader coverage loss at 4.8 million by 2034, with 18.5 million people subject to compliance documentation each year.
The Arkansas experience from 2018 is the data point nobody wants to revisit: after implementing work requirements, 18,164 people lost coverage in the first six months. The majority were already working. They simply could not navigate the documentation portal.
Data point: 18.5 million Medicaid expansion enrollees will need to document work compliance monthly starting January 2027. KFF analysis finds 80 percent of the target population already works. The barrier is documentation, not employment.
2. The Uncompensated Care Cascade
Here is the mechanism that most financial models undercount.
When patients lose Medicaid, they do not stop needing care. Chronic disease does not respect policy timelines. A diabetic who loses coverage in October 2026 still needs insulin in November. A pregnant woman who cannot navigate a work documentation portal still delivers in January. A patient with hypertension who is red-flagged at redetermination still has hypertension.
They show up at the FQHC. They have to. The FQHC is legally required to see them.
NACHC estimates this law will add approximately $7 billion per year in higher costs from uncompensated care for community health centers, plus an additional $6 billion in broader economic impact, for a total of $13 billion annually.
That $7 billion is not a cut. It is a cost that appears without corresponding revenue.
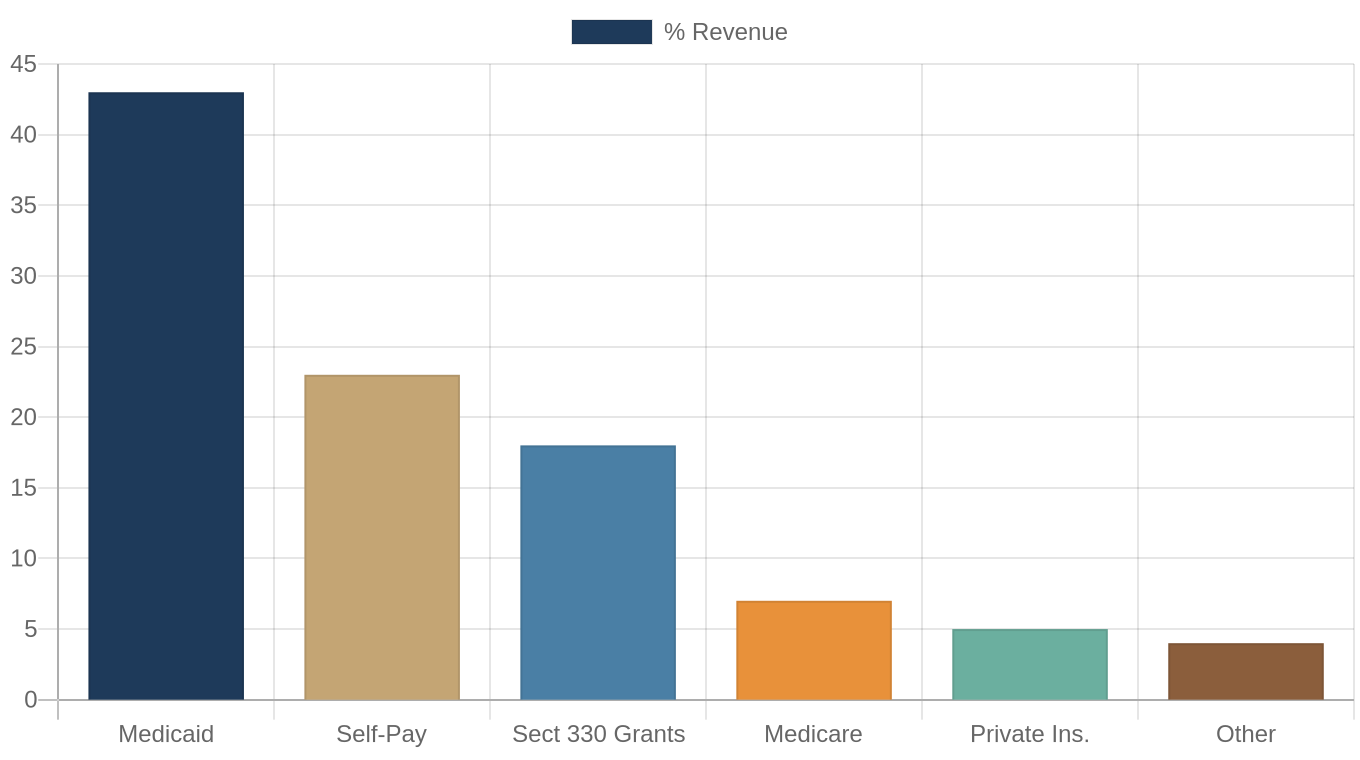
Medicaid currently accounts for approximately 43 percent of FQHC operating revenue - more than any other single source. When patients lose coverage and return as self-pay or sliding-scale patients, the revenue follows a one-way downward ratchet. Same patient. Same visit. A fraction of the payment.
A Medicaid visit reimburses at $300 to $400 on average. A sliding-scale visit at an FQHC runs $15 to $50. The clinical cost is identical. The reimbursement differential is the difference between a financially solvent health center and one in distress.
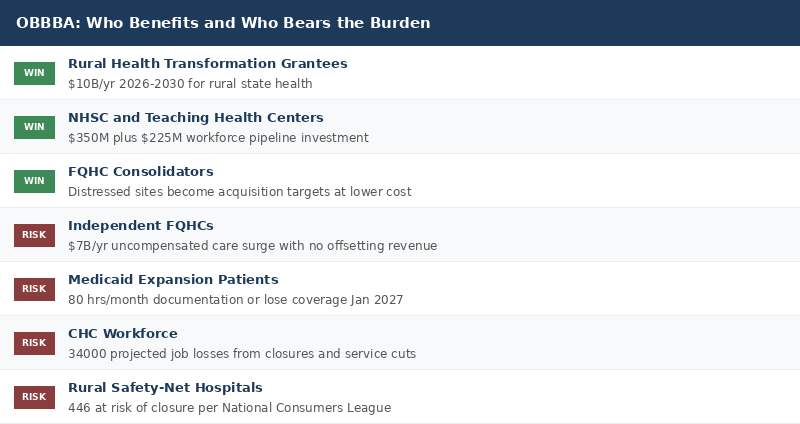
NACHC projects the total economic impact will lead to at least 34,000 CHC job losses and 1,800 CHC site closures. Those sites are not in well-resourced markets. They are the only primary care option in rural counties, agricultural communities, and urban neighborhoods with no other safety-net providers.
Data point: NACHC projects 1,800 community health center site closures and 34,000 job losses from the combined revenue contraction under OBBBA.
3. The Funding Paradox: A Silver Lining Inside the Reckoning
Here is the part the headlines consistently miss.
OBBBA did not cut Section 330 grant funding. In fact, the Community Health Center Fund was set at $4.6 billion for FY 2026 - which NACHC described as the largest increase to the CHCF in a decade. The law also provides $350 million in base funding for the National Health Service Corps, $225 million for Teaching Health Center Graduate Medical Education, and a Rural Health Transformation program providing $10 billion per year from 2026 through 2030.
These are real investments. They matter for workforce pipeline and rural access. But here is the math problem.
A $4.6 billion CHCF increase does not offset a $7 billion per year uncompensated care surge. The grant fund increase is a one-time authorization level. The uncompensated care surge is compounding and structural. Medicaid represents 43 percent of FQHC revenue - more than double the next-largest source. No grant increase in the single-digit billions can hedge a 43-percent revenue source contracting.
The Rural Health Transformation program is similarly complicated. Ten billion dollars per year flowing through state allotments for rural health interventions sounds significant. But it is distributed across 50 states, directed to prevention and chronic disease programs, and does not flow directly to FQHC operations or patient care costs. It supplements. It does not replace.

Data point: The $4.6 billion Community Health Center Fund increase - the largest in a decade per NACHC - covers approximately 18 percent of average FQHC revenue. It cannot offset a 43 percent revenue source contracting.
4. State-Level Asymmetry
The OBBBA creates profoundly unequal impact across states - and the states with the most vulnerable populations are absorbing the worst of it.
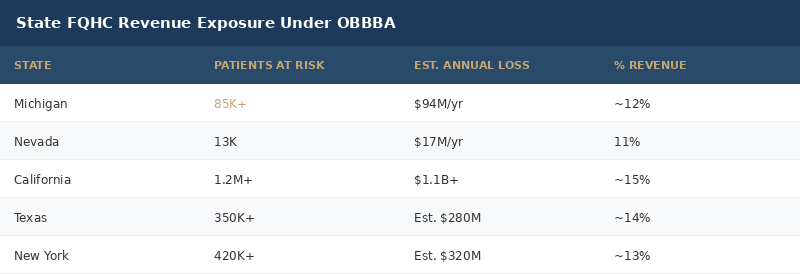
Michigan FQHCs project losing $94 million in reimbursement annually, per the Michigan Primary Care Association. Nevada FQHCs project losing $17 million per year - 11 percent of their operating revenue - affecting 13,000 patients.
States that expanded Medicaid have a particular exposure. They built entire care systems on the assumption of a 90 percent federal match rate for expansion populations. When that enhanced FMAP ended on January 1, 2026, states faced a choice: absorb the additional cost or reduce eligibility. For states running tight fiscal balances, the pressure toward eligibility reduction is structural, not optional.
The geographic pattern matters. The states with the largest FQHC patient populations - California, Texas, New York, Florida, and Illinois - are also the states with the most complex political and fiscal dynamics around Medicaid expansion. The communities most exposed are the ones FQHCs were built to serve.
5. The Retroactive Coverage Trap
One provision that receives less attention than it deserves is the retroactive coverage window change.
Under prior law, a Medicaid expansion enrollee could receive up to two months of retroactive coverage - meaning care received before their application was processed could be covered retroactively. Under OBBBA, that window is now one month for expansion enrollees.
The practical effect: there is a predictable coverage gap around the moment of enrollment - exactly when patients are most likely to be presenting for care. The scenario that seeded this newsletter is not hypothetical. A pregnant woman presents for a prenatal visit, applies for Medicaid, and the visit that prompted the enrollment is no longer covered. The cost falls on her or the FQHC.
Multiplied across millions of enrollees, that single month represents hundreds of millions of dollars in previously-covered care now falling into the uncompensated column. For FQHCs running negative net margins - the median CHC net margin in 2024 was -2.1 percent - this is not an edge case. It is a recurring structural hit on each new enrollee.
Data point: More than 16 million of the 35 million patients served annually by community health centers are Medicaid-insured. Every additional coverage gap month for new enrollees compounds directly into FQHC uncompensated care burden.
Deep Dive: The Three-Year FQHC Financial Scenario
Here is how the math works for a medium-sized FQHC - five clinic sites, 50 providers, 100,000 annual patient visits - roughly the median CHC organization profile.
Year 1 (2026): Noncitizen and Redetermination Hit
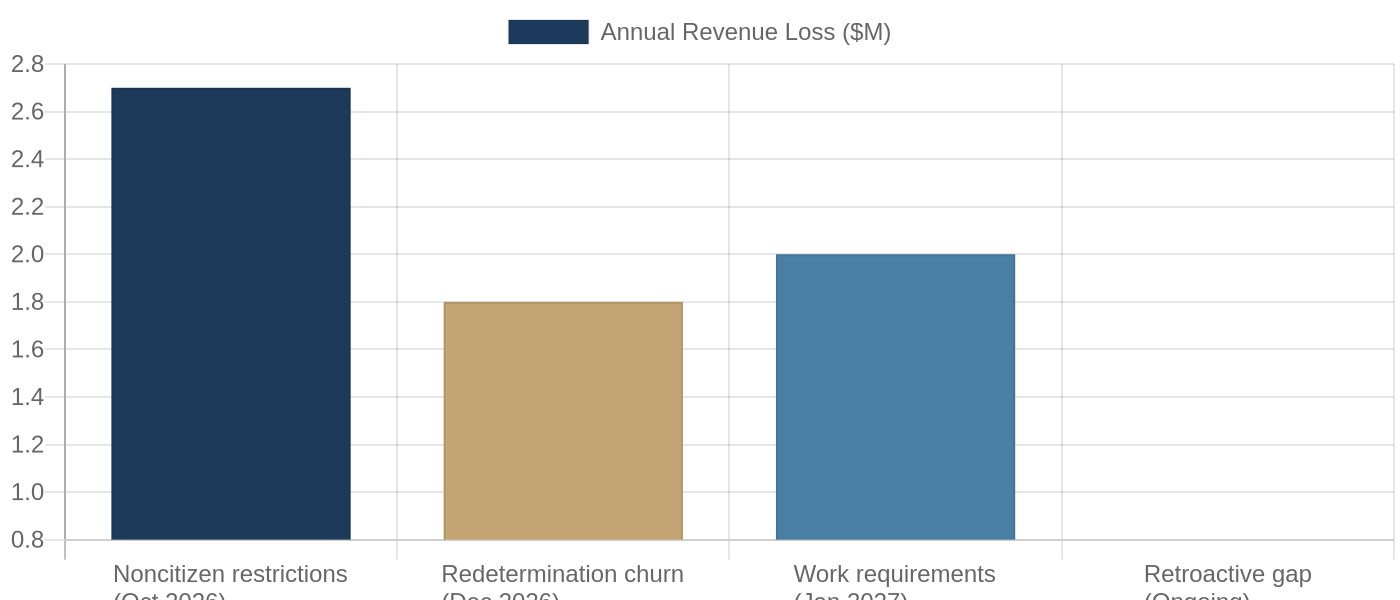
Assume 8 percent of the patient panel are noncitizen patients who lose coverage by October 1. At 100,000 annual visits, that is 8,000 visits shifting from Medicaid to uninsured. Revenue loss at a $335 per-visit differential: $2.7 million per year.
Redetermination churn adds a second layer. Assume 20 percent temporary disenrollment of the technically-eligible panel, with 75 percent eventually reinstated. Net permanent and semi-permanent loss: roughly 5 percent of the Medicaid panel. Additional revenue loss: approximately $1.8 million per year.
Total Year 1 impact: -$4.5 million on an organization with $25 to $35 million in annual revenue. That is a 13 to 18 percent operating revenue reduction in year one.
Year 2 (2027): Work Requirements Layer In
Work requirements become enforceable January 1, 2027. Applying NACHC's 5.6 million at-risk national figure proportionally to a 100,000-visit organization places roughly 10,000 annual visits at risk.
Assume 40 percent successfully navigate compliance documentation. The remaining 60 percent lose coverage. That is 6,000 visits shifting from Medicaid to uninsured, adding $2.0 million per year in additional revenue loss.
Cumulative Year 2 annual impact: -$6.5 million per year.
Year 3 (2028+): Compounding Effects
By year three, the cumulative revenue contraction begins triggering operational consequences. Reduced Medicaid panel shrinks efficient care management programs. Cost per visit rises as the uninsured panel requires more social work, navigation, and interpreter services per encounter.
Site consolidation is triggered. One to two of five sites close or reduce to part-time operations. Remaining sites absorb displaced patient volume with fewer resources. Staff turnover accelerates as wage pressure mounts.
The organizations that navigate this three-year compression will be those that modeled it in 2026 - before the full impact landed.
What This Means For You
For FQHC and community health center leaders: Audit your noncitizen patient percentage now. Coverage loss for that cohort begins October 1, 2026. Invest in Medicaid application navigation and redetermination support before December 31. Patients who lose coverage in the paper shuffle but remain technically eligible are recoverable with adequate staff resources. Model your three-year cash flow under scenario B and scenario C. Your board needs to see the downside cases now, not after the revenue contraction is already in the numbers. Contact your state Primary Care Association to understand your state's redetermination implementation timeline and any state-level buffers available.
For health system administrators and CMOs: Emergency department volumes will rise proportionally to FQHC site closures. This is documented from every prior coverage contraction. Build formal care partnerships or shared navigation services with local FQHCs before they enter financial distress. The relationship is easier to build now. Identify which FQHCs in your referral network are financially fragile. Do that assessment now while partnerships are still possible.
For radiologists, pulmonologists, and specialists: FQHC patients represent the highest concentration of unscreened high-risk individuals for lung cancer, cardiovascular disease, and chronic respiratory conditions. Site closures mean those patients lose the care coordinators who refer them to you. For lung cancer specifically: Stage I survival is 77 percent. Stage IV is 9 percent. An unscreened FQHC patient who loses their care navigator in 2027 is a Stage IV presentation in 2029.
For healthcare investors and founders: 1,800 projected site closures represent a significant market dislocation. Distressed FQHC assets, patient panels, and workforce become available at non-premium prices. Revenue cycle AI, sliding-scale billing optimization, and Medicaid navigation tools have a clear and urgent buyer base in the safety-net market right now. The $10 billion Rural Health Transformation program is a policy tailwind for rural-focused models - but the window to build rural relationships before the funding hits is closing.
For policy advocates: State-level legislative and regulatory action on redetermination processes is the highest-leverage near-term advocacy target. State implementation choices remain contestable. 34,000 projected CHC jobs represent a coalition-building opportunity across labor and health advocacy communities.
The Closing Argument
There is a version of this story where the OBBBA's investments in rural health, workforce training, and the Community Health Center Fund partially offset the damage. The $4.6 billion CHCF increase is real. The Rural Health Transformation program funding is real. NACHC's acknowledgment of the CHCF increase as the largest in a decade is accurate.
But the $7 billion annual uncompensated care surge is also real. And it is not offset by grant increases. It is structural volume growth against a revenue base that just got carved out.
The communities absorbing this are not abstract policy populations. They are the 35 million patients who use community health centers as their primary care home. They are the rural counties where the nearest alternative to an FQHC is a 90-minute drive. They are the agricultural worker who cannot document 80 hours of work per month because the documentation portal only exists in English.
The OBBBA passed. The implementation clock is running.
What are you doing before December 31?
Jonathan Govette is the Co-Founder and CEO of Oatmeal Health, an AI lung cancer diagnostic company catching cancers earlier in the communities that need it most. Oatmeal uses AI to identify unscreened high-risk patients, navigate them to care, and score every lung CT for malignancy risk - billed under CPT 0721T. Stage I survival is 77%. Stage IV is 9%. We work in FQHCs because that gap is largest there.
Jonathan writes daily about radiology, pulmonology, AI diagnostics, health policy, hospital operations, and healthcare startups. Subscribe to stay ahead of healthcare's most important shifts at oatmealhealthjonathangovette.substack.com
Key References: National Consumers League: The Impact of the One Big Beautiful Bill Act on Healthcare Accessibility Nationwide (July 7, 2026) - https://nclnet.org/impact-of-h-r-1-on-healthcare-accessibility/ | NACHC: State Impacts of the One Big Beautiful Bill - https://www.nachc.org/state-impacts-of-the-one-big-beautiful-bill/ | Feldesman Tucker: The One Big Beautiful Bill Act Is Approved By the Senate - https://www.feldesman.com/the-one-big-beautiful-bill-act-is-approved-by-the-senate-devastating-impacts-for-health-coverage-overall-some-silver-linings-for-fqhcs/ | KFF: Work Requirement Provisions in the 2025 Federal Budget Reconciliation Law - https://www.kff.org/medicaid/a-closer-look-at-the-work-requirement-provisions-in-the-2025-federal-budget-reconciliation-law/ | AMA: Changes to Medicaid and the ACA under H.R.1 - https://www.ama-assn.org/health-care-advocacy/federal-advocacy/changes-medicaid-aca-and-other-key-provisions-one-big