

Medicare GLP-1 Bridge Program
Starting July 1, Medicare pays $50 a month for Wegovy and Zepbound - but 82% of eligible seniors don't know it yet, and a documentation trap is already waiting for them.


The coverage wall just cracked.
Starting July 1, 2026, Medicare will do something it has never done in its 61-year history. It will pay for GLP-1 medications prescribed specifically for weight management - not for diabetes, not for cardiovascular risk reduction as a secondary diagnosis, but for obesity itself.
For two decades, federal law explicitly banned Medicare Part D from covering drugs used solely for weight loss. That was not an accident. It was a deliberate policy choice, written into statute and defended through every budget cycle since 2003. On July 1, that choice ends.
The Medicare GLP-1 Bridge Program gives eligible seniors access to Wegovy, Zepbound, and Foundayo at a $50 monthly copay. Medicare negotiated the price down from $1,000 to $1,350 per month to a $245 net per-month supply. The federal government absorbs the difference.
It is a bigger deal than the coverage it provides. It is a signal that Washington now officially treats obesity as a disease worth treating - and that the $1.3 trillion annual cost of cardiovascular disease projected by 2050 is a problem worth disrupting upstream.
But here is the part that should alarm every health system, FQHC, and primary care practice in the country: 82% of Medicare beneficiaries do not know this is happening. The program starts in two days. Most eligible seniors will not walk through the door asking for it. That means the burden falls on you - and your documentation workflow had better be ready.

1. Two Decades of Exclusion, Now Over
When Medicare Part D was created in 2003, Congress included a blanket prohibition on covering drugs used "for anorexia, weight loss, or weight gain." The legislative rationale was that obesity treatments were not proven effective and that covering them would balloon the Part D budget.
That rationale aged badly. The clinical evidence that has accumulated since 2020 makes it indefensible. Semaglutide (Wegovy) produces an average 13.7% reduction in body weight in patients without diabetes. Tirzepatide (Zepbound) produces 20.2% weight reduction. The SELECT trial - 17,604 adults with obesity but no diabetes - demonstrated that Wegovy reduces major adverse cardiovascular events by 20%.
These are not lifestyle drugs. They are disease-modifying agents with peer-reviewed outcomes data published in the New England Journal of Medicine. The FDA cleared Wegovy for secondary cardiovascular risk reduction. Zepbound received clearance for obstructive sleep apnea. These are the exact populations that fill Medicare rolls.
The Treat and Reduce Obesity Act (TROA) passed through the House Committee on Ways and Means with bipartisan support and has made legislative progress toward removing the permanent statutory exclusion. The Bridge Program is CMS's immediate bridge: an 18-month demonstration running July 1, 2026 through December 31, 2027, using a demonstration authority that sidesteps the Part D prohibition without waiting for Congress to finish the job.
The mechanics are deliberately simple. The Bridge operates entirely outside the standard Part D benefit structure. Part D plans carry zero risk for these prescriptions. Humana - already running the Limited Income Newly Eligible Transition (LI NET) program - serves as the central processor for claims adjudication and pharmacy payment. Patients use their Medicare card, pay $50, and the pharmacy gets reimbursed by a parallel track.
For providers, the operational implication is critical: your patients do not need to switch plans, file appeals, or navigate a new insurance portal. They walk into the pharmacy with their existing Part D card and a valid prior authorization. Which brings us to the piece of this program that is most likely to generate denials.
2. Who Qualifies: The Clinical Matrix and Its Gaps
Eligibility for the Medicare GLP-1 Bridge is specific, tiered, and documentation-dependent. There are three pathways:
Pathway 1 - BMI of 35 or greater (no comorbidity required). This is the broadest pathway. If your patient is a Medicare Part D enrollee with a BMI at or above 35, they qualify on BMI alone.
Pathway 2 - BMI of 30 or greater with qualifying comorbidity. Qualifying conditions are: heart failure, uncontrolled hypertension, or chronic kidney disease stage 3a or higher. A patient with a BMI of 31 and a CKD diagnosis qualifies. A patient with a BMI of 31 and controlled hypertension does not.
Pathway 3 - BMI of 27 or greater with high-risk cardiovascular diagnosis. Qualifying conditions are: prediabetes, prior myocardial infarction, prior stroke, or symptomatic peripheral artery disease. This pathway has the most clinical specificity and the most room for documentation error.
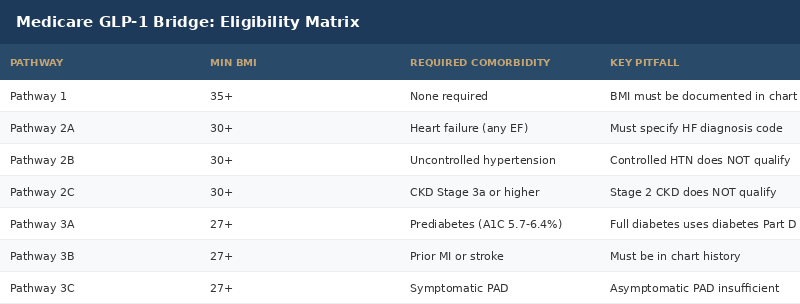
The eligibility language contains real traps. "Uncontrolled hypertension" is not defined by a specific blood pressure threshold in the Bridge guidance - but payers will look for documentation supporting that characterization. Prediabetes must be documented, not just inferred from A1C. And BMI must be in the chart at the time of the prescription.
One more requirement that many providers have missed: patients must be enrolled in a lifestyle modification program focusing on diet and physical activity. This is a condition of certification. If a provider submits a prior authorization without documenting that the patient is participating in a lifestyle program, the authorization may be denied or pended.
3. The Prior Authorization Problem: Retrospective, Not Prospective
The Bridge Program uses retrospective prior authorization. Providers prescribe the medication first. The documentation, diagnosis codes, BMI measurement, and comorbidity verification are submitted after the prescription is written.
On its surface, this sounds patient-friendly - no waiting for approval before the patient starts treatment. In practice, it creates a different problem. Retrospective PA means clinics that do not front-load their documentation will face post-hoc denials. The pharmacy will dispense the medication. The patient will take it. And then a denial arrives in the mail weeks later, triggering retroactive cost recovery from either the pharmacy or the patient.
The prior authorization form is submitted electronically or by fax to Humana's central processor. CMS has published a standardized form. Every field matters. The system has no tolerance for ambiguity in comorbidity documentation.
📊 CMS has certified that providers must submit: BMI documentation from a clinical encounter within the prior 12 months; diagnosis codes for all qualifying comorbidities; attestation that the patient is enrolled in a lifestyle modification program; and a prescription from a licensed prescriber. Missing any of these components creates a denial pathway even if the patient is clinically eligible.

4. The 82% Problem: Who Is Not Going to Show Up
Here is the most important number in this story: 82%.
That is the share of Medicare beneficiaries who, according to a June 2026 survey by the Obesity Care Advocacy Network, are unaware that Medicare is about to begin covering GLP-1 medications for weight management. The survey covered more than 2,100 adults ages 65 and older, and the findings held across party lines - 79% of Republicans and 84% of Democrats were equally uninformed.
CMS deliberately limited its public outreach ahead of July 1. The agency's reasoning: beneficiaries are "most moved to take action" when a benefit is actually available, not when it is announced in advance. That approach may be defensible from a behavioral economics standpoint. It is problematic from an access equity standpoint.
More than 69% of Medicare beneficiaries are overweight or obese - 35% classified as overweight, 34% as obese. Among those classified as obese, 28% already have Type 2 diabetes. CBO estimates that 29 million Medicare beneficiaries would qualify for weight management GLP-1 coverage under an expanded policy. The Bridge program does not reach all 29 million - the eligibility criteria are more restrictive - but the potential eligible population remains enormous.
The patients who will show up on July 2 asking for this benefit are the patients who read health news, have engaged physicians who flag it proactively, or are being cared for at systems that built a workflow for it. The patients who will not show up are the patients in underserved communities, rural counties, and safety-net clinics, whose providers are stretched thin and whose outreach infrastructure is minimal.
📊 Only 9% of adults ages 65 and older are currently using GLP-1 medications. That number does not move without proactive provider identification of eligible patients.
5. The Racial and Equity Gap Inside the Bridge
Obesity is not evenly distributed in America. Black Americans have the highest obesity prevalence of any racial group, followed by Hispanic adults. The populations most burdened by the disease that this program treats are also the least likely, historically, to receive GLP-1 prescriptions.
A 2026 study published in Obesity found that non-Hispanic white patients were the most likely to be prescribed a long-acting GLP-1 at 2.4%, compared to 2.3% for non-Hispanic Black patients, 1.8% for Hispanic patients, and 1.7% for Asian patients. These differences appear small in absolute percentage terms, but they represent hundreds of thousands of patients across the Medicare population.
The disparities are not random. They reflect differential access to obesity medicine specialists, primary care capacity, insurance coverage history, and provider bias. A 2026 analysis found that provider bias and weight stigma mean physicians are statistically less likely to discuss weight-loss treatments with patients from lower-income or minority backgrounds - even when clinical criteria are met.
There is evidence that policy interventions can close this gap. Research on state Medicaid policies that expanded GLP-1 coverage found that racial and ethnic prescription disparities decreased significantly after coverage expanded. The Bridge Program, by reducing cost to $50 per month, removes the largest single barrier. But cost is not the only barrier.
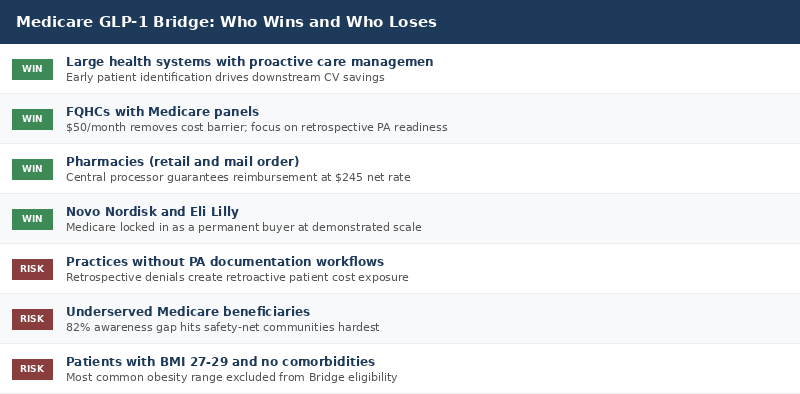
For FQHCs serving predominantly Black and Hispanic Medicare patients, the Bridge Program is an immediate clinical and operational opportunity. The question is whether those clinics have the bandwidth and the workflow to execute.
6. The Business Case for Health Systems
The Medicare GLP-1 Bridge creates real downstream financial implications for health systems beyond the drug cost itself.
CBO projects that expanded GLP-1 coverage for Medicare beneficiaries could save $3.4 billion in healthcare costs through 2034 by reducing heart attacks, strokes, diabetes complications, and other obesity-related conditions. The mechanism is straightforward: treat obesity now, avoid expensive acute events later.
For health systems managing large Medicare populations, this is a portfolio bet on reducing acute utilization. A patient on Wegovy for 18 months who avoids one hospitalization for a cardiac event saves the system far more than the drug cost.
The financial model for a mid-size health system illustrates the stakes.
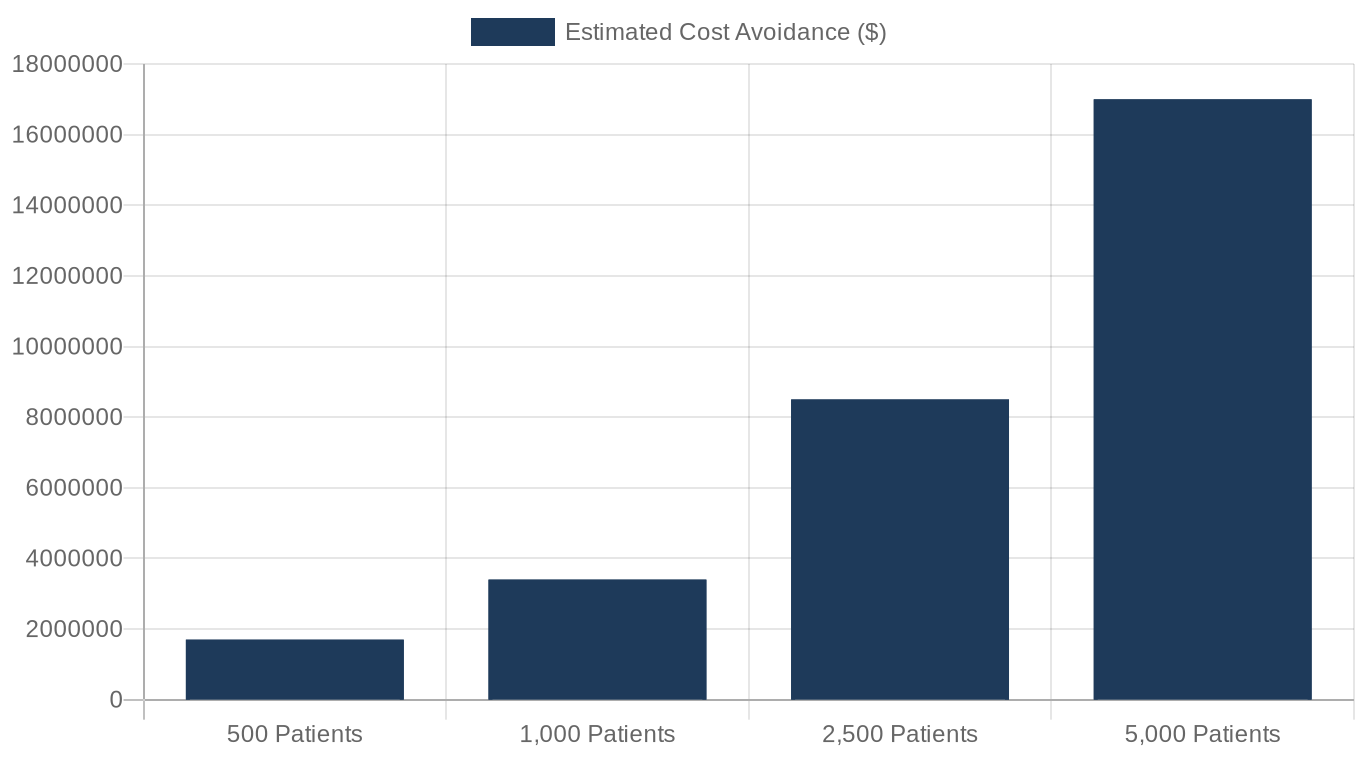
Note: Estimated at $3,400 per patient in downstream cardiovascular savings based on CBO projections normalized to the 2026 eligible population. These are illustrative ranges, not actuarial guarantees.
7. Deep Dive: The Drug Landscape and What Providers Need to Know Today
The Medicare GLP-1 Bridge covers three specific products beginning July 1. Understanding the distinctions matters for prescribing decisions.
Foundayo (tirzepatide, Eli Lilly) - an oral tirzepatide formulation, cleared specifically for weight management. The first oral GLP-1/GIP dual agonist available in the Bridge. Patients who cannot tolerate injections now have an oral option.
Wegovy (semaglutide, Novo Nordisk) - available in injection and tablet formulations. The SELECT trial cardiovascular outcomes data supports its use in patients with established cardiovascular disease and obesity without diabetes. The oral formulation (Rybelsus re-branded as Wegovy tablet for weight management) is now included.
Zepbound KwikPen (tirzepatide, Eli Lilly) - the injectable formulation covered under the Bridge. SURMOUNT-OSA Phase 3 data showed significant reduction in apnea-hypopnea events, making this particularly relevant for Medicare patients with comorbid sleep apnea.
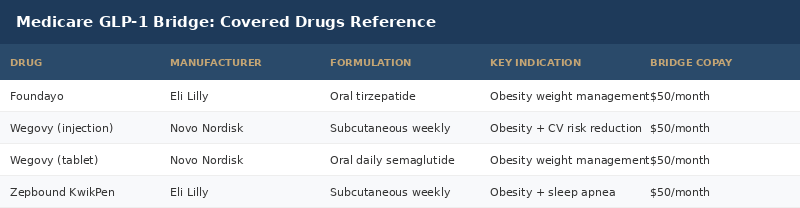
What is NOT covered under the Bridge:
Ozempic (semaglutide for diabetes) and Mounjaro (tirzepatide for diabetes) remain outside the Bridge because they carry diabetes indications, not weight management indications. If a patient has diabetes and obesity, the diabetes indication governs and the Bridge does not apply. Those patients use existing Part D diabetes drug coverage.
This distinction will cause confusion at the point of prescribing. Providers need to verify which formulation and indication they are prescribing under before submission.
The Lifestyle Program Requirement
The requirement that patients be enrolled in a lifestyle modification program is real and enforceable. CMS defines a qualifying program as one that focuses on dietary change and physical activity, supervised or supported by a licensed healthcare professional. A printed handout is not sufficient documentation. A documented referral to a formal program or a structured internal clinic protocol with defined touchpoints is.
For FQHCs, this is actually an opportunity. Many already operate diabetes prevention programs and behavioral health integration models that qualify as lifestyle modification programs under this definition. Documenting the Bridge lifestyle requirement alongside an existing DPP enrollment can create a clean audit trail.
Prior Authorization: The Exact Steps
1. Patient visit: Document BMI in the chart from this encounter or within prior 12 months. 2. Confirm qualifying pathway and document diagnosis codes. 3. Document lifestyle program enrollment. 4. Generate prescription for qualifying Bridge drug. 5. Submit PA request electronically or by fax to the Humana central processor using the CMS-issued form. 6. Humana adjudicates, notifies prescriber and pharmacy. 7. Patient fills prescription at any participating pharmacy for $50.
The retrospective nature means the PA form can be submitted after the prescription is written, but it should ideally be submitted the same day to minimize any gap between dispensing and authorization.
8. What This Means for the Permanent Coverage Question
The Bridge is temporary. December 31, 2027 is the hard end date. What happens after that is not settled.
The BALANCE Model - CMS's broader demonstration architecture that was supposed to include a permanent Part D weight management component - has had its Part D component delayed indefinitely. The Bridge itself was extended through December 2027 precisely because the BALANCE Model was not ready.
The permanent solution requires legislation. The Treat and Reduce Obesity Act (TROA) provides the statutory pathway by removing the longstanding Part D exclusion language. With bipartisan support in committee and the clinical evidence now undeniable, legislative passage is more likely than at any point in the program's history.
But "more likely than ever" and "certain" are different. If the Bridge ends in December 2027 without TROA passage, patients who started Wegovy or Zepbound under the Bridge face an abrupt coverage cliff. The cardiovascular and metabolic benefits of these medications are dependent on sustained use - stopping creates rebound weight gain and risk restoration. A coverage cliff for 29 million potentially eligible beneficiaries is not a policy nuance. It is a public health event.
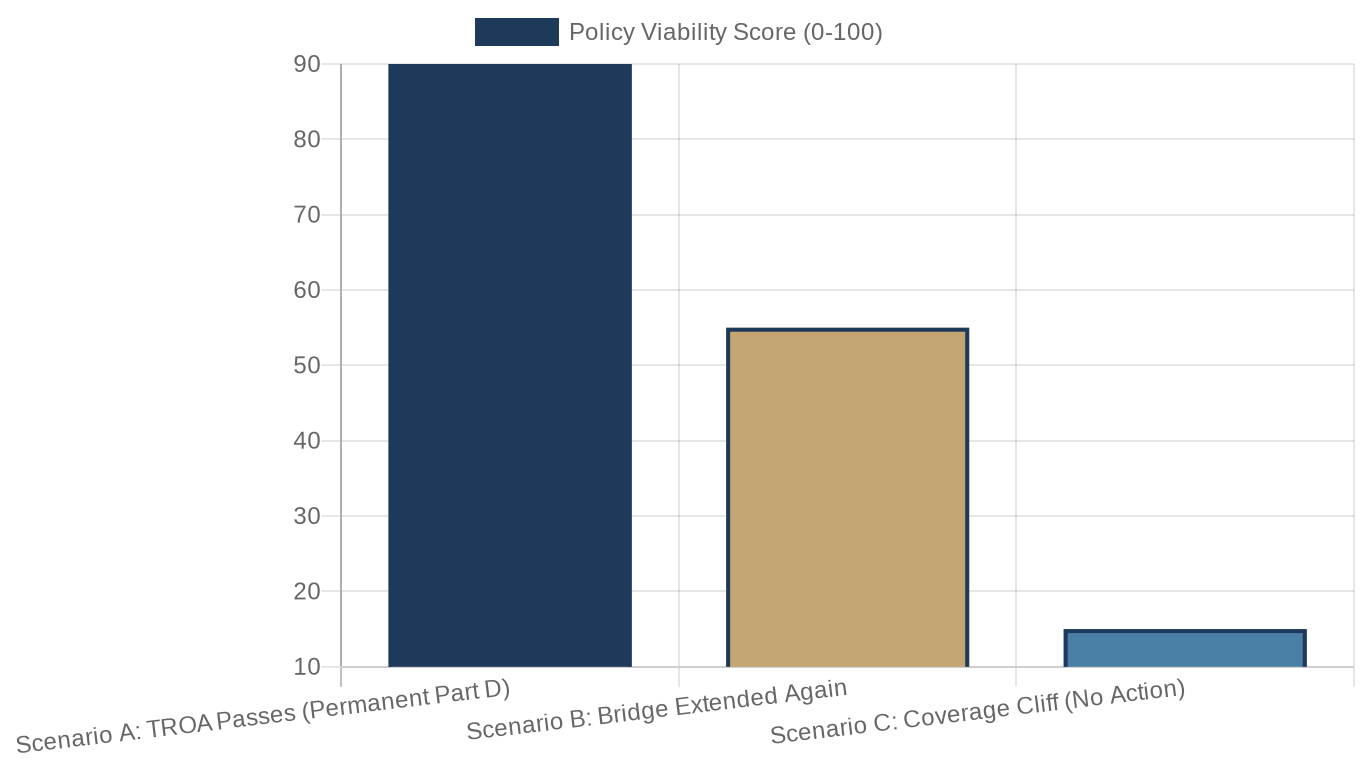
Note: Scores reflect analyst consensus on likelihood and health system impact from Georgetown and STOP Obesity Alliance policy analyses, not CMS projections.

What This Means for You
If you are an FQHC or community health center CEO: Your Medicare patient panel is the first place the Bridge creates real opportunity and real risk. Identify your patients with BMI 30+ and qualifying comorbidities now, before they show up without a workflow to receive them. Stand up your lifestyle program documentation today. The July 1 start date is not a planning horizon. It is a deadline.
If you are a health system CMO or Chief Medical Officer: The Bridge is an 18-month window to demonstrate that proactive obesity management reduces acute utilization. Build the identification and outreach protocol now. This is the kind of downstream savings demonstration that payers and boards pay attention to. Do not wait for patients to self-identify.
If you are a primary care physician: Get the CMS prior authorization form from the Medicare GLP-1 Bridge provider portal before you write your first Bridge prescription. The retrospective PA process is forgiving if you have the form ready. It is expensive if you do not. Verify which drug you are prescribing under - Bridge indications and standard Part D indications are not interchangeable.
If you are a radiologist or pulmonologist: Your patients with severe obesity and sleep apnea (Zepbound's additional indication) are some of the highest-BMI patients in your panel. They are also among the most likely to qualify under Pathway 2 or 3. Adding Bridge eligibility screening to your pre-procedure documentation workflow adds minimal burden for potentially significant patient benefit.
If you are a healthcare investor or founder: The Bridge is a 18-month forced experiment in what happens when you dramatically lower the cost of GLP-1s for Medicare seniors. The utilization data, outcomes data, and cost savings data generated through December 2027 will be the most powerful evidence base the obesity medication market has ever had. Watch it carefully. Whatever the Bridge proves will shape permanent coverage policy for decades.
If you are a policy advocate: The clock is ticking on TROA. The Bridge buys time but does not fix the statute. Every month that passes without a permanent legislative solution is a month closer to a coverage cliff that will hit the patients who can least absorb it.
Closing
There is a sentence worth sitting with today.
For 61 years, Medicare did not treat obesity as a disease worth treating. The evidence was weak, the drugs were limited, and the policy consensus held. Then the clinical evidence became undeniable. The drugs became transformative. And Congress moved slowly anyway.
The Medicare GLP-1 Bridge is what happens when an administration decides not to wait. It is imperfect - time-limited, eligibility-restricted, documentation-dependent, and under-publicized. It will not reach everyone who needs it. The 82% awareness gap ensures that the patients with the least access will get the least benefit.
But the coverage wall cracked. And the physics of policy change are such that cracks tend to widen.
The real question for every health system, FQHC, and primary care practice in America is not whether this program changes the landscape. It is whether your organization is positioned to get your patients through the opening before it closes - or before it becomes permanent.
Are your documentation workflows built for July 1?
About the Author
Jonathan Govette is the Co-Founder and CEO of Oatmeal Health, an AI lung cancer diagnostic company catching cancers earlier in the communities that need it most. Oatmeal uses AI to identify unscreened high-risk patients, navigate them to care, and score every lung CT for malignancy risk - billed under CPT 0721T. Stage I survival is 77%. Stage IV is 9%. We work in FQHCs because that gap is largest there.
Jonathan writes daily about radiology, pulmonology, AI diagnostics, health policy, hospital operations, and healthcare startups.
Subscribe to stay ahead of healthcare's most important shifts. Weekly deep-dives on AI, radiology, health policy, FQHCs, and the business of healthcare - written for operators, clinicians, and investors who want the signal, not the noise. Subscribe at oatmealhealthjonathangovette.substack.com