

Medicaid Work Requirements Miss the Mark
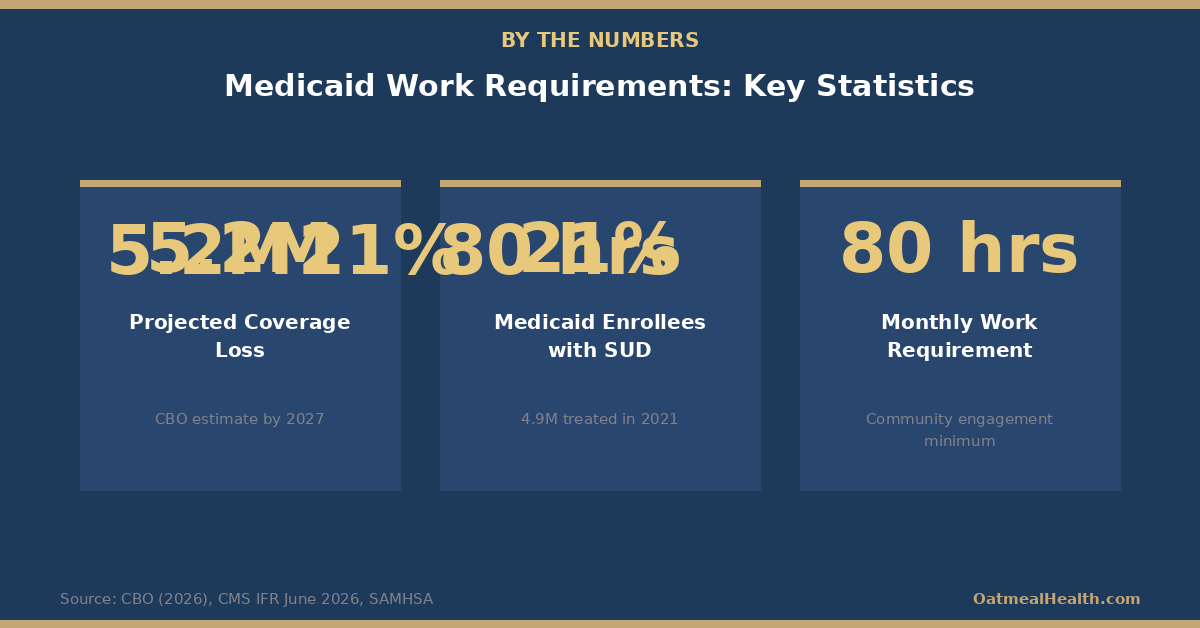
New federal rules create a five-year recovery cliff for SUD patients, with the CBO projecting 5.2 million coverage losses by 2027.


Something shifted in American healthcare policy on June 1, 2026. That day, the Centers for Medicare and Medicaid Services (CMS) issued an Interim Final Rule establishing Medicaid community engagement requirements as national policy. By July 31, the rule takes effect. By January 1, 2027, 44 states and the District of Columbia must begin implementation.
Nebraska didn't wait. It launched the country's first Medicaid work requirement program on May 1, 2026, before the federal rule even dropped. The template was set, and the rest of the country is now following.
At its core, the policy sounds simple: Medicaid enrollees who are able to work must spend 80 hours per month on work, community service, education, or job training to keep their coverage. Fail to document that time, and you lose Medicaid, at least temporarily.
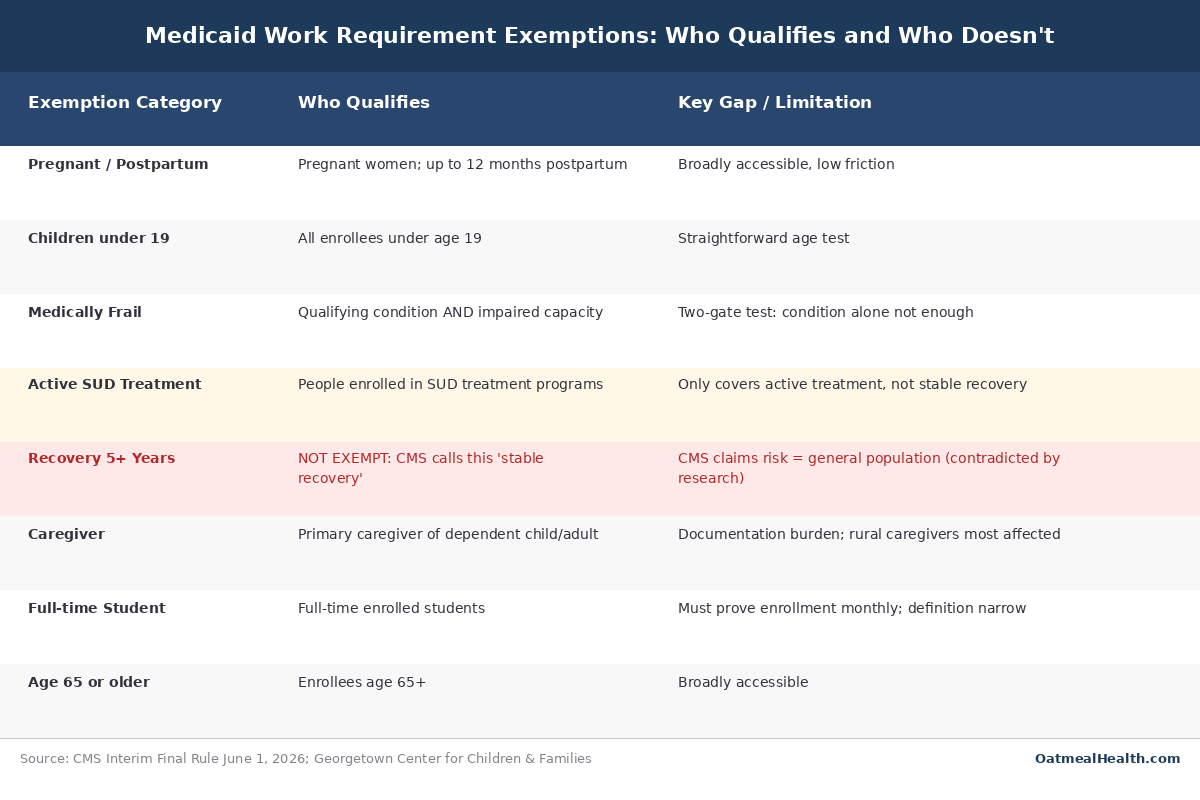
The exemptions sound generous: pregnant women, children, caregivers, students, people over 65, and people with serious medical conditions. The rule's architects argue it targets only those who are genuinely able to work and simply aren't engaging.
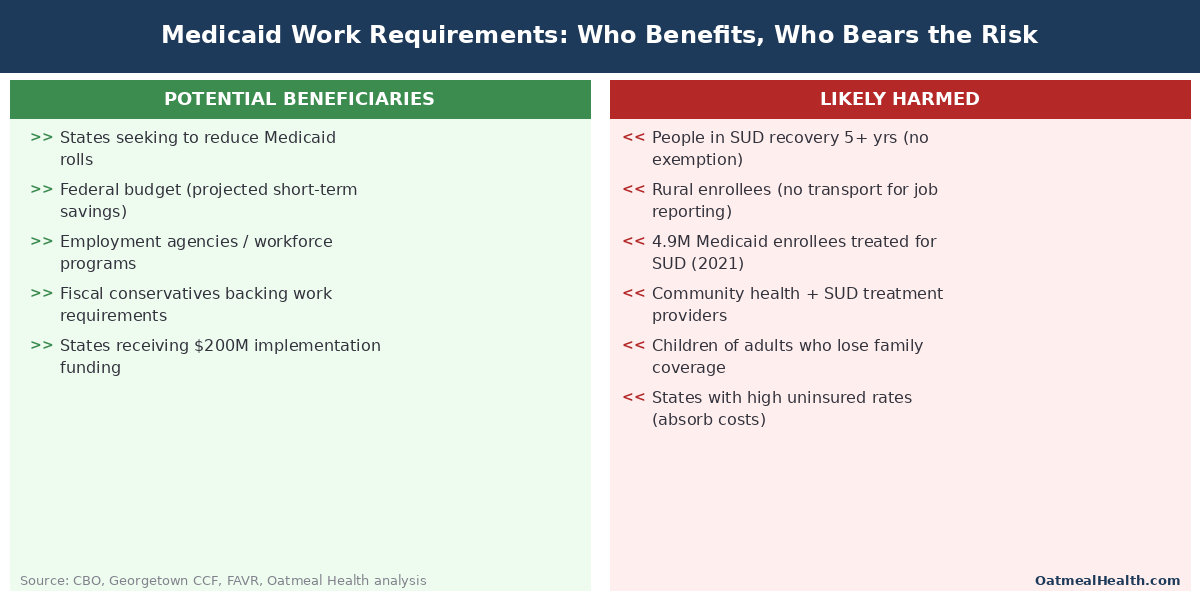
But a close look at the exemption structure, the science of addiction recovery, and the only prior experiment with Medicaid work requirements reveals a different story. This rule is likely to strip coverage from millions of people who are genuinely ill, including hundreds of thousands managing substance use disorders, not because they won't work, but because the documentation system will fail them, or because the exemption they need doesn't apply to them the way it sounds like it should.
The Rule That Is Already Reshaping Medicaid
The One Big Beautiful Bill Act authorized Medicaid community engagement requirements as part of a broader fiscal package. CMS's June 1 Interim Final Rule translates that authority into specific requirements.
Enrollees between ages 19 and 64 who are not exempt must complete 80 hours per month of qualifying activity. This can include paid work, volunteer work, job training, or education. States must build compliance reporting systems to verify participation monthly, a significant administrative undertaking.
Implementation funding is available: $200 million to CMS and $200 million distributed to states, split evenly between equal allocation and population-based allocation. Larger states receive meaningfully more resources to build compliance infrastructure.
The comment period for the rule closes July 31, 2026, the same day it takes effect. That simultaneity has drawn sharp criticism from health policy advocates, who argue it prevents meaningful public input before states begin spending resources on implementation.
The SUD Exemption: A Five-Year Cliff
The most consequential design flaw in this rule isn't the 80-hour requirement itself. It's what happens to people with substance use disorders after five years of recovery.
The medically frail exemption uses a two-gate test. An enrollee must first have a qualifying condition, then separately demonstrate that the condition impairs their capacity to meet the work requirement. Both gates must be cleared. A serious diagnosis alone is not enough.
For people with substance use disorders, the exemption is further narrowed by a hard cutoff. CMS treats people in stable recovery of five or more years as carrying the same health risk as the general population. After that five-year mark, the SUD-based pathway to the medically frail exemption closes.
This is where the science and the policy diverge sharply.
Faces and Voices of Recovery (FAVR), a national advocacy organization, published a detailed critique of the IFR in July 2026. Their analysis is direct: addiction is a chronic, relapsing brain disease. The five-year mark does not represent a biological reset after which vulnerability to relapse drops to general population levels. Long-term recovery is real progress, but it is maintained through ongoing behavioral, social, and sometimes medical support. Loss of health coverage is precisely the kind of destabilizing event that elevates relapse risk.
Georgetown University's Center for Children and Families (CCF) has raised a parallel concern about the two-gate medically frail structure. People in unstable housing, without reliable transportation, or in early treatment engagement are the least likely to successfully navigate a monthly documentation process. The complexity of the test creates barriers that fall hardest on the most vulnerable enrollees.
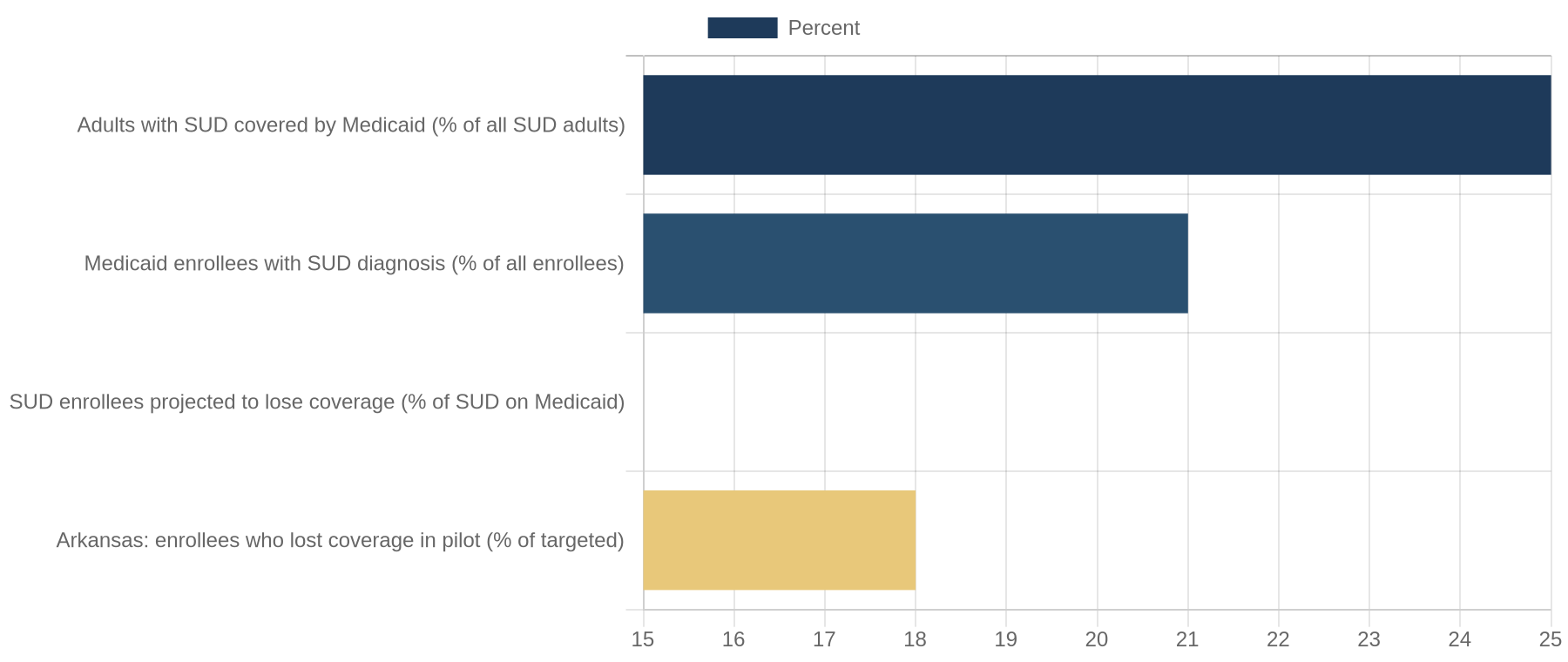
The scale of the population affected is significant. An estimated 4.9 million Medicaid enrollees received treatment for substance use disorders in 2021. Approximately 21 percent of all Medicaid enrollees have an SUD diagnosis. Medicaid is the single largest payer for addiction treatment in the United States, covering roughly 25 percent of all adults with substance use disorders. This population is central to the program, not peripheral.
What the Numbers Show
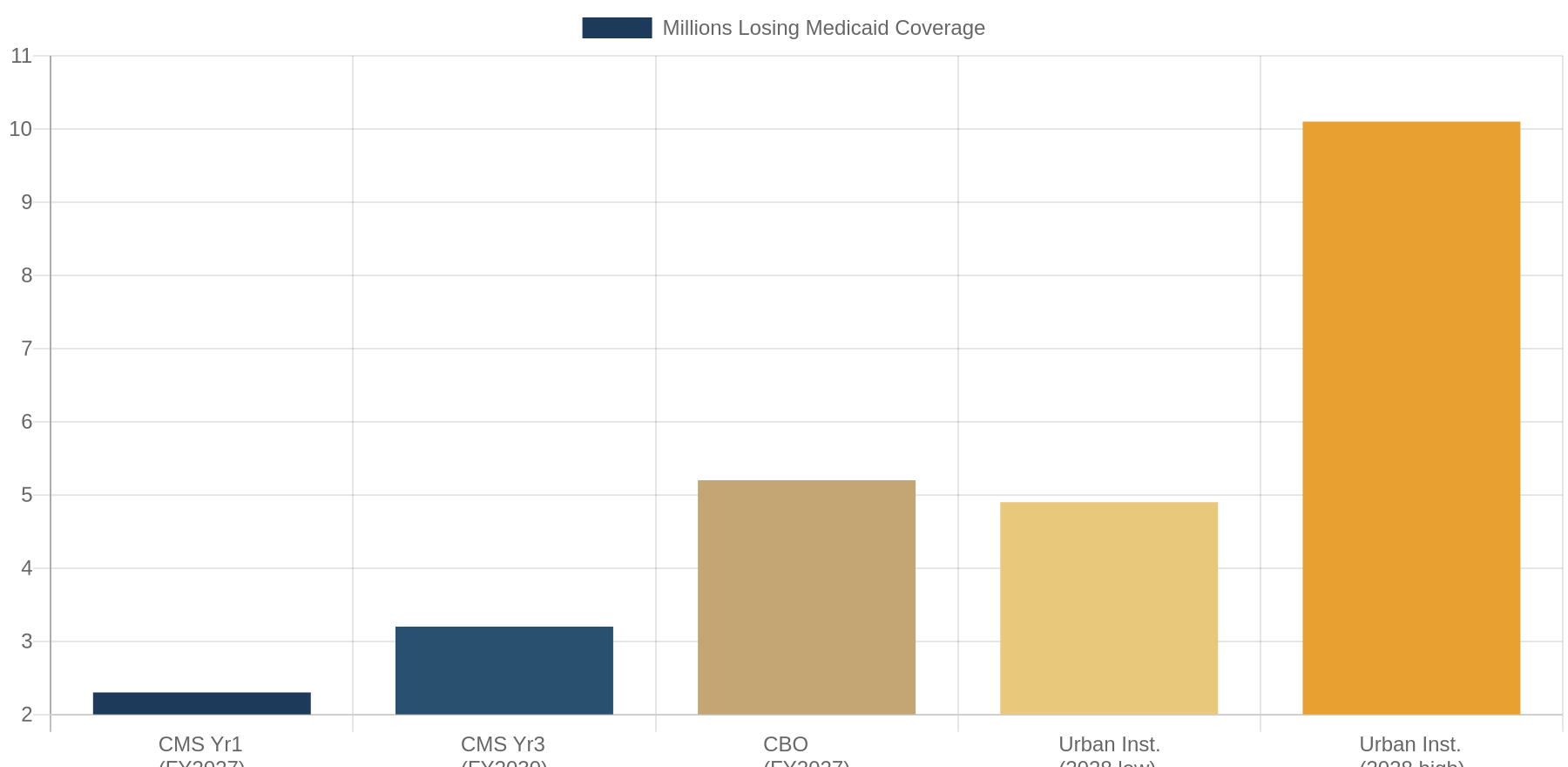
Three major analytical bodies have modeled the coverage impact of Medicaid work requirements. Their estimates differ in methodology, but all point the same direction.
The Congressional Budget Office projects that work requirements will cause 5.2 million people to lose Medicaid coverage by 2027, potentially rising to 10 million by 2034. Critically, the CBO finds that most who lose coverage will have actually met the work requirement. They will lose coverage because they failed to document compliance, because the reporting system created barriers, or because they weren't reached by outreach.
The Urban Institute estimates 4.9 to 10.1 million people losing coverage by 2028, depending on how aggressively states enforce reporting and how much administrative friction they build into their processes.
Even CMS's own IFR projections acknowledge substantial coverage losses: 2.3 million disenrolled in FY2027, growing to 3.1 to 3.3 million by FY2030. These are the federal government's own numbers.
The pattern across all three analyses is important: the coverage losses aren't primarily driven by people who fail to meet the work requirement. They're driven by people who can't navigate the documentation system. This distinction matters for policy design. A work incentive that causes eligible people to lose coverage because of paperwork is not a work incentive. It is a coverage reduction mechanism.
The Arkansas Warning, Eight Years Later
We don't have to model all of this in the abstract. In 2018 and 2019, Arkansas implemented the country's first Medicaid work requirement under a federal waiver. The results are a matter of record.
Within six months, 18,000 adults lost Medicaid coverage. A follow-up study published in the New England Journal of Medicine found that work requirements did not increase employment among Arkansas Medicaid enrollees. The people who lost coverage were not people who got jobs. They were people who couldn't navigate the monthly reporting system, didn't know the requirement existed, or faced technical barriers to online documentation.
The downstream health effects were measurable: 56 percent of those who lost coverage reported delaying medical care, and 64 percent reported delaying medications because of cost. These are not people who decided they were healthy enough to go without insurance. They were cut off from care they needed and couldn't afford to replace it.
A federal court halted the Arkansas program in January 2019, ruling that CMS had not properly considered whether the program furthered Medicaid's statutory objective of providing medical assistance. The legal doctrine from that case has since evolved, which is partly why CMS believes the current IFR is legally defensible. But the policy outcomes from Arkansas are unchanged.
Work requirements, as implemented, did not produce more workers. They produced more uninsured people.
The State Directed Payment Problem
Buried in the same rulemaking package is a provision that deserves more attention: caps on State Directed Payments (SDPs) for Medicaid services.
State Directed Payments allow states to direct Medicaid managed care organizations to pay higher rates to specific provider categories, often community health centers, safety-net hospitals, and behavioral health and SUD treatment providers. These payments have been critical to keeping addiction treatment infrastructure viable in states where standard Medicaid reimbursement rates would otherwise be insufficient.
The proposed SDP caps could reduce reimbursement to exactly the providers who serve people most at risk under work requirements. The combination is significant: remove coverage from people in SUD recovery by closing the exemption after five years, then reduce reimbursement to the providers most likely to treat them if they retain coverage. SUD provider associations have begun raising this interaction, but it remains underreported relative to the headline coverage loss projections.
What Happens After July 31
The July 31 effective date creates an unusual policy window. The rule is in effect but most states haven't implemented it yet. Comments are being received but no regulatory response is required before implementation begins. Legal challenges are anticipated but may not receive initial rulings before the first states go live in the fall of 2026.
Organizations including FAVR, Georgetown CCF, the National Health Law Program, and state-level Medicaid advocacy coalitions are submitting comments and monitoring for legal intervention opportunities. What advocates are asking for, at minimum, is a meaningful SUD exemption that reflects the chronic, relapsing nature of addiction rather than an arbitrary five-year cutoff, plus procedural protections: advance notice, appeal rights, and a meaningful cure window before coverage terminates.
Whether those asks get traction before states begin implementation is an open question. The political dynamics that produced this rule haven't changed. But the empirical record, from Arkansas, from the CBO analysis, and from the addiction science literature, is clear and consistent.
The Bottom Line
Medicaid work requirements are now federal policy. The debate over whether they should exist is, for the moment, settled at the federal level. The debate over how they're designed is not.
The specific choices embedded in this IFR, the five-year SUD cliff, the two-gate medically frail test, the monthly documentation burden, the simultaneous comment and effective date: these are not inevitable features of a work requirement. They are design choices. And they are choices with predictable, documented failure modes.
The Arkansas data is eight years old, and it already showed us exactly what happens when the compliance infrastructure can't match the complexity of real people's lives. People who met the work requirement still lost coverage. People in genuine medical need still lost coverage. The coverage losses didn't produce employment gains.
None of this proves that community engagement requirements are impossible to design well. It means this particular design has well-documented vulnerabilities. The comment period is open until July 31. The implementation clock is running.
If 5.2 million people lose Medicaid coverage, the majority of them will have been eligible. They'll have lost it on paperwork.
Sources: Faces and Voices of Recovery (FAVR), July 2026 Monthly Policy Update | CMS Interim Final Rule, June 1, 2026 | Congressional Budget Office Score of the One Big Beautiful Bill Act | Georgetown University Center for Children and Families Medicaid Analysis | Urban Institute Medicaid Coverage Loss Projections | NEJM: Arkansas Medicaid Work Requirement Outcomes Study (2019) | SAMHSA National Survey on Drug Use and Health (2021)