

FQHC Funding: Bandage on a Wound
Congress is promoting a $50 billion rural health program while simultaneously cutting the core grants and Medicaid funding that keep 1,800 community health centers open.


The headline said it plainly: "New Rural Health Funding Only a Bandage for Medicaid Wound."
That is not an editorial opinion. That is a cash flow analysis.
Congress is promoting a $50 billion Rural Health Transformation Program. The number is large enough to generate a White House announcement and warm applause at health center conferences. Average first-year state awards are running $200 million. Some states are putting forward thoughtful implementation plans. The political optics are good.
But look at what is happening at the same time. The Community Health Center Fund - the Section 330 grant program that has been the foundational operating support for federally qualified health centers for decades - was extended only through December 2026. No long-term authorization. No inflation adjustment. Just a short runway over a cliff.
And Medicaid, which accounts for 43 percent of FQHC operating revenue nationwide, is being cut by a projected $911 billion over 10 years under the One Big Beautiful Bill. Work requirements alone are projected to cause 5.6 million community health center patients to lose Medicaid coverage over five years.
Three legs of the FQHC financial stool - Section 330 grants, Medicaid reimbursement, and 340B drug savings - are all under simultaneous pressure. A $50 billion rural program that reaches only some health centers in some states is not a solution to that math. It is a headline pasted over a structural failure.

1. What the Rural Health Transformation Program Actually Does - and Does Not Do
The Rural Health Transformation Program is real money. $50 billion over five fiscal years, $10 billion per year, from 2026 through 2030. It is allocated to approved states, with half divided equally among all states and half weighted by rural population, number of rural health facilities, and related factors.
The program is designed to support Critical Access Hospitals, rural health clinics, FQHCs receiving Section 330 grants that serve rural populations, and certain behavioral and mental health providers. CMS has begun awarding first-year funding, with state awards averaging $200 million in year one.
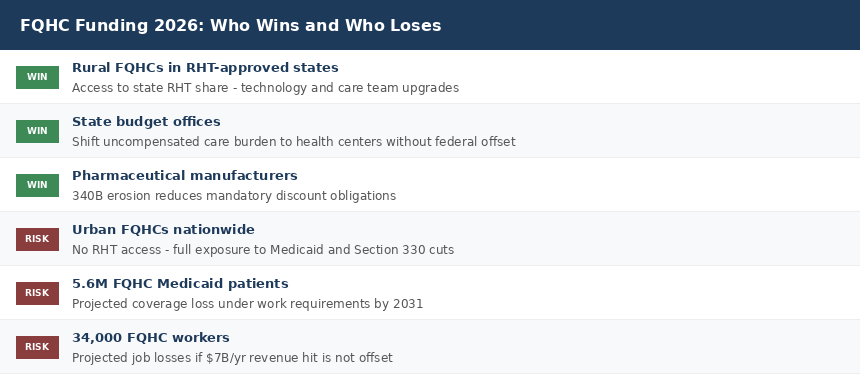
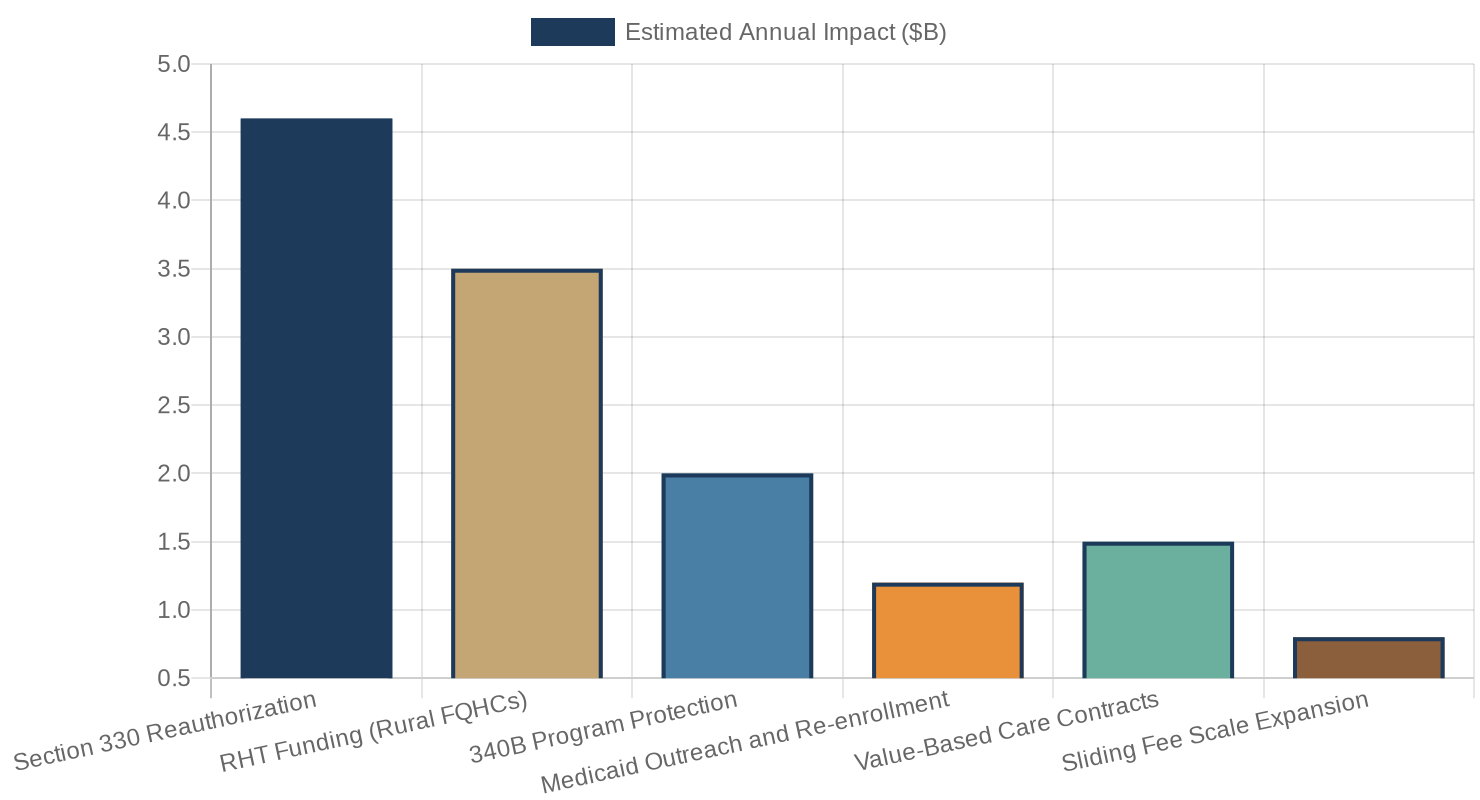
Some states are putting RHT funds to immediate use. Delaware is investing in an "FQHC Value-Based Care Readiness" initiative covering technology upgrades, expanded care teams, and care management infrastructure. That is the right kind of use for this funding.
📊 First-year RHT state awards average $200M - spread across all rural health entities in a state, not directed exclusively to FQHCs.
Here is the structural problem. The Rural Health Transformation Program helps rural FQHCs in approved states. That is a meaningful subset of the community health center system. It is not the whole system.
There are approximately 1,400 federally qualified health centers operating more than 14,000 service delivery sites across the country. A significant share of them are in urban and suburban areas - serving the same Medicaid-dependent, uninsured, and underinsured patient populations as their rural counterparts. They face the same financial pressure. They get nothing from RHT.
More fundamentally, the Rural Health Transformation Program is a new grant program layered on top of the existing funding structure. It does not replace Section 330. It does not replace Medicaid reimbursement. It does not protect 340B. It adds a new revenue stream for a limited subset of health centers while the three foundational revenue streams continue to erode.
The Authorization Cliff
The Community Health Center Fund was authorized through December 2026 by the Consolidated Appropriations Act signed in early 2026. That $4.6 billion in FY2026 funding is real support. But the authorization cliff at year-end creates a crisis that health center administrators are already managing right now.
Hiring decisions cannot wait until December to know whether funding continues. Capital investments in new sites or equipment require multi-year confidence in revenue. Workforce planning for clinical staff - physicians, nurse practitioners, dentists, behavioral health providers - operates on 18 to 24 month time horizons.
When Section 330 authorization ends at December 2026 with no successor legislation, health centers do not wait to see what Congress does. They stop hiring in October. They delay site expansions. They hold staff positions open rather than filling them. The damage from funding uncertainty arrives before the funding actually stops.
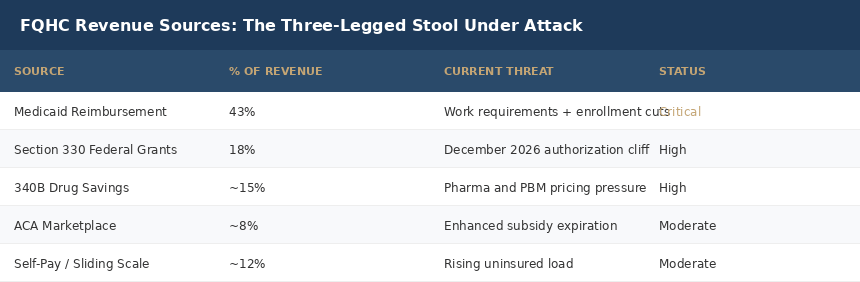
2. The Three-Legged Stool
Community health center finance is built on three structural revenue sources. Remove any one of them and a health center's operating model strains to its limit. Remove two simultaneously and you are talking about closures, not adjustments.
Leg One: Medicaid
Medicaid is the single largest payer for community health centers, accounting for 43 percent of operating revenue on average. More than 16 million CHC patients carry Medicaid coverage. When those patients lose coverage, they do not disappear from the health center - they show up as uncompensated care.
The One Big Beautiful Bill included $911 billion in Medicaid spending reductions over 10 years. The most direct impact on community health centers comes from two provisions working in combination.
First, work requirements. Adults ages 19 to 64 in Medicaid expansion states must now document at least 80 hours per month of work or qualifying activity as a condition of eligibility, effective no later than December 31, 2026. Arkansas tried this in 2018. In six months, 18,164 people lost coverage. Most of them were already working. The paperwork infrastructure to document eligibility did not exist, and eligible patients could not navigate the online portal.
NACHC projects that over five years, nearly 5.6 million CHC Medicaid patients in expansion states could lose coverage under these requirements. That translates to direct revenue loss for health centers - and an offsetting surge in uncompensated care for the same facilities.
📊 5.6 million CHC Medicaid patients projected to lose coverage over 5 years under the new work requirements.
Second, per capita caps and enrollment restrictions. As states implement coverage changes and as enhanced ACA marketplace subsidies that expired at the end of 2025 push more patients back to uninsured status, the paying patient mix at health centers shifts sharply toward nonpaying. Health centers are legally required to serve anyone regardless of ability to pay. The operating model assumes a sustainable ratio of paying to nonpaying patients. When that ratio breaks, the model breaks with it.
Leg Two: Section 330 Grants
Section 330 of the Public Health Service Act has been the federal backbone of community health center funding since 1965. These grants currently total approximately $4.6 billion annually and are distributed through HRSA directly to health centers.
The grants fund services that are not fully reimbursed through Medicaid or private insurance - behavioral health services, dental care, pharmacy services, transportation coordination, case management, and enabling services. These are the services that most differentiate a federally qualified health center from a standard primary care clinic. They are also the services most likely to catch a lung cancer screening referral, a maternal mental health flag, or a patient drifting off their chronic disease management plan.
When grant funding is uncertain, these enabling services are the first to be cut. The services most vulnerable are often the most important for population health outcomes in underserved communities.
📊 $4.6 billion in Section 330 grants currently support 14,000 FQHC service delivery sites - authorized only through December 2026.
Leg Three: 340B
The 340B Drug Pricing Program, established in 1992, requires pharmaceutical manufacturers participating in Medicaid to sell outpatient drugs to eligible safety-net providers at deeply discounted prices - typically 20 to 50 percent below market rates. Community health centers are among the core eligible entities.
340B savings do not sit in a reserve fund. They subsidize the services that Medicaid and grant funding do not fully cover. They allow a health center to maintain an on-site pharmacy and dispense medications to patients who cannot afford to fill a prescription at a retail pharmacy. They fund the care coordination staff who prevent $50,000 emergency hospitalizations.
The 340B program is under sustained attack from multiple directions at once. Pharmaceutical manufacturers are restricting contract pharmacy arrangements - the mechanism through which FQHCs access 340B pricing through external pharmacies. Pharmacy benefit managers have introduced billing and reimbursement practices that erode the effective discount. On Capitol Hill, proposals circulate to tighten eligibility or restrict how savings can be used.
None of these threats has individually dismantled 340B. Together, they are compressing the margins that health centers depend on to serve patients who cannot pay full freight.
3. The Urban FQHC Is Being Left Out
The Rural Health Transformation Program creates a structural bifurcation in the community health center system. Rural FQHCs in approved states can potentially access RHT funding. Urban FQHCs cannot.
This matters because urban patient populations at community health centers are not categorically healthier, wealthier, or less dependent on safety-net services than rural populations. A health center in South Chicago or East Los Angeles or North Philadelphia serves patients with the same clinical complexity, the same Medicaid dependency, and the same lack of alternatives as a center in rural Mississippi.
The policy logic of prioritizing rural health is understandable. Rural hospital closures are accelerating. Provider shortages in rural areas are severe. The public health statistics in rural communities are dire. Investment is warranted.
But the framing of "rural health investment" as a counterweight to broader Medicaid cuts does not hold up at the aggregate level. The Medicaid cuts affect health centers in Chicago as hard as they affect health centers in rural Vermont. The Section 330 authorization cliff hits every health center equally. The 340B erosion is not confined to rural settings.
A policy that offers targeted rural investment while cutting the universal funding mechanisms is a net negative for the system as a whole, even if some rural centers individually come out ahead.
4. What Is Already Happening on the Ground
The closures and service reductions are not hypothetical. They are already in progress.
In New Hampshire, a rural FQHC announced the closure of one of its sites in late 2025, citing a projected operating shortfall driven by Medicaid funding changes. In South Carolina, an FQHC closed six locations and transferred services to other agencies, citing financial pressure and a rising share of uninsured and underinsured patients.
These closures are happening before the Section 330 authorization cliff, before Medicaid work requirements fully take effect in December 2026, and before ACA marketplace subsidy loss converts additional newly insured patients back to uninsured status.
One in four community health centers currently faces a negative operating margin. NACHC projects that without increased funding, one in four may close or reduce services over the next two years.
📊 1 in 4 community health centers currently operates at a negative financial margin.
The compounding timeline matters. December 2026 is when Section 330 authorization expires. That is also when Medicaid work requirements must be implemented nationwide. That is also the end of a year in which ACA marketplace subsidies have already been eroding since enhanced subsidies expired at the end of 2025. Three major financial stressors are converging at the same calendar point.
Health center administrators are not waiting to see what happens. They are making decisions right now about what they will be able to operate in 2027.
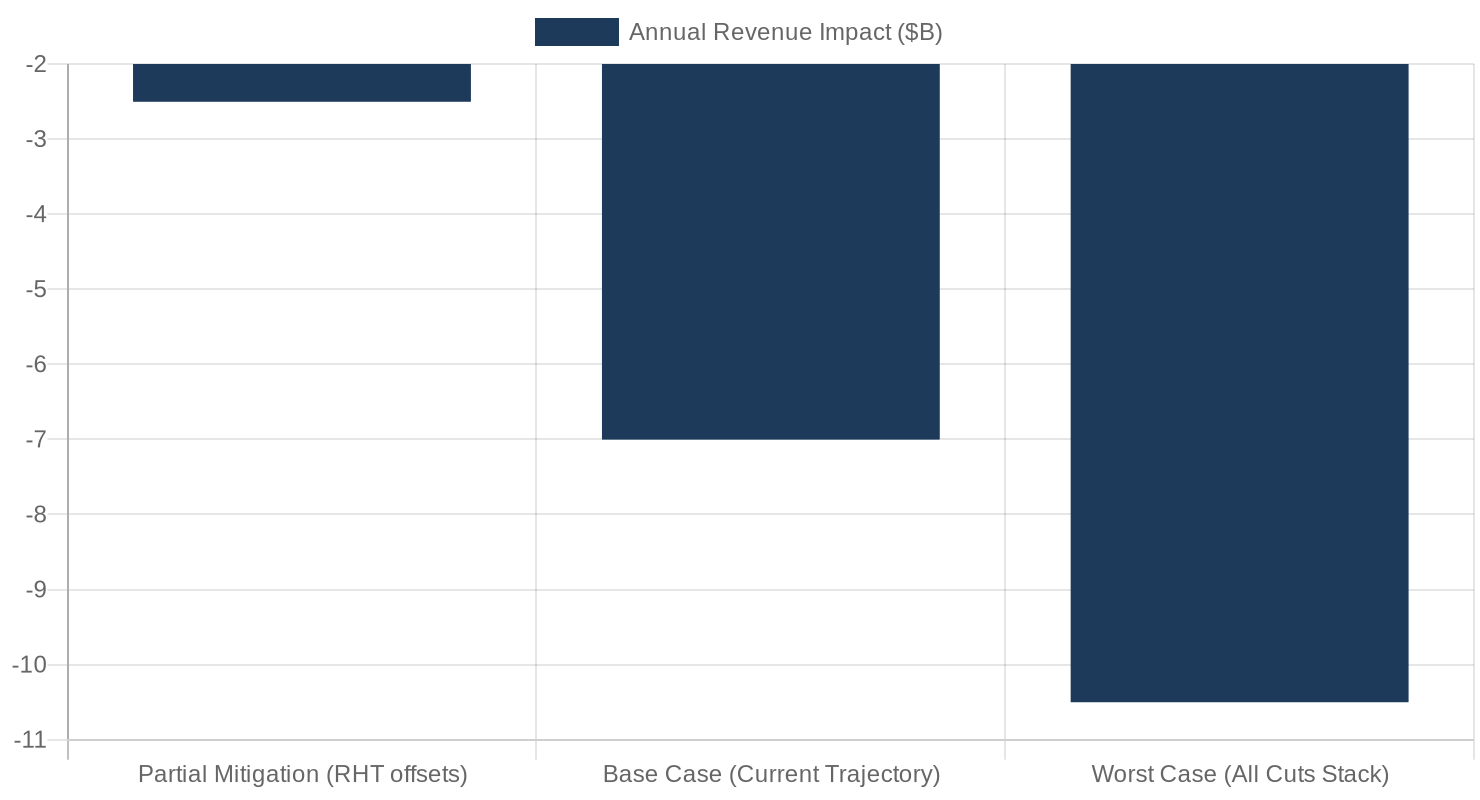
5. The Three-Scenario Financial Model
Community health center financial planning in 2026 requires modeling three distinct scenarios, because the policy environment is genuinely uncertain across all three funding legs.
Scenario A: Partial Mitigation
RHT funding flows efficiently to rural health centers. Section 330 is reauthorized in early 2027 at current funding levels. Medicaid work requirement implementation is slower than projected due to state administrative delays. Net revenue loss to the system runs approximately $2 to 3 billion annually. Health centers in this scenario survive but cut enabling services, reduce hours at some sites, and defer capital investment.
Scenario B: Base Case - Current Trajectory
Section 330 authorization lapses in December 2026 for several months before a continuing resolution restores it at flat funding. Medicaid work requirements reduce coverage for millions of patients starting in mid-2027. 340B pressures continue to compress savings. Annual system revenue loss reaches approximately $7 billion - the NACHC projection. Approximately 1,800 FQHC sites close or reduce to appointment-only operations. 34,000 jobs are eliminated. 32 million current patients see reduced access.
Scenario C: Compounding Worst Case
Section 330 lapses without a quick continuing resolution. Medicaid work requirements are implemented on schedule with higher than projected coverage loss. A legislative change to 340B further restricts program savings. Annual system revenue loss exceeds $10 billion. Urban health centers face disproportionate closures because they have no RHT offset.
Deep Dive: The Mechanics of an FQHC Closure
Health centers do not close overnight. They close over 18 months of deferred decisions that accumulate until the operating model fails. Understanding the sequence is essential for any health system leader, policy advocate, or investor trying to intervene before the announcement.
It typically starts with a hiring freeze. A nurse practitioner leaves and the position stays open. A medical director announces retirement and the replacement search is put on hold. Each open clinical position reduces visit capacity by 15 to 20 percent.
Then the enabling service cuts begin. Transportation coordination goes first - it generates no fee revenue and requires dedicated staff time. Dental services get reduced to emergency extractions because the dental hygienist position cannot be refilled. Behavioral health visits are capped at six per patient per year instead of 12. The pharmacy closes on Fridays.
By the time a community health center announces a closure, the community has already been losing access for a year. The announcement is the last domino, not the first.
📊 The typical FQHC closure sequence: hiring freeze at month 1, enabling service cuts at month 6, site consolidation at month 12, formal closure announcement at month 18.
For health system administrators tracking referral patterns: a health center announcing a hiring freeze in the context of funding uncertainty is the intervention window. Not the closure announcement. When a health center in your community enters this sequence, your emergency department is going to absorb those patients in about 18 months. Model that volume now.
For anyone who has watched what happens to communities after FQHC closures: the primary care access gap takes years to fill. Private practices do not open in rural counties with median incomes under $35,000. Urgent care chains do not follow communities into the neighborhoods that community health centers serve. The patients who depended on that health center end up in emergency departments for primary care conditions, or they simply do not get care at all.
The patients who do not get care are the ones most likely to present with late-stage disease. At Oatmeal Health, we work every day on the gap between lung cancer detection and lung cancer survival. Stage I survival is 77 percent. Stage IV is 9 percent. The difference between those outcomes is often a care coordinator who was on staff at a community health center - until the hiring freeze in month one.
What This Means For You
For FQHC executives and community health center leaders: Run your three-scenario financial models now. Model Section 330 authorization lapsing at December 2026 and not returning until March 2027. Model Medicaid volume declining 10 to 20 percent in your panel starting mid-2027. Identify which enabling services you can sustain on Medicaid and grant revenue alone - and which require 340B savings to operate. If you are a rural FQHC in a state that received RHT funding, engage your state Medicaid agency now about how health center investment is being prioritized in the application.
For health system administrators and CMOs: FQHC closures redirect medically complex, socially vulnerable patients to your emergency department. Model this volume now. A rural health center closure typically generates a 15 to 30 percent increase in ED utilization from its former patient panel. That is documented from prior closure events, not an estimate. Plan your capacity and care navigation resources accordingly.
For radiologists and pulmonologists: The patients most likely to present with late-stage lung cancer are the same patients who receive primary care at FQHCs. If Section 330 grant cuts eliminate care coordination roles at community health centers, patients who were on track for LDCT lung cancer screening at age 50 will not get screened. The FQHC is often the only access point between a high-risk patient and a scan that saves their life.
For healthcare investors and founders: The FQHC financial crisis creates urgent demand for solutions that reduce administrative burden. Revenue cycle optimization tools, Medicaid eligibility re-enrollment platforms, population health management infrastructure, and telehealth models that allow health centers to serve more patients with fewer staff are addressing real and growing problems. The market need is validated, immediate, and expanding.
For policy advocates: The comment period for the CMS Medicaid managed care proposed rule remains open. Submitting real operating financial data from actual health centers - not projections, but audited financials - is the most effective form of policy engagement at this stage. NACHC coordinates this effort. The July 21, 2026 comment deadline is the next immediate opportunity.
The closing point is this. The rural health investment in the Rural Health Transformation Program is real and in some communities it will make a meaningful difference. States that invest RHT funds in FQHC technology infrastructure and care model transformation are making the right call.
But policy math is not about intentions. It is about net outcomes.
When Section 330 authorization expires at year-end, when Medicaid work requirements strip coverage from millions of patients starting December 31, 2026, and when 340B savings continue to erode - the net outcome for the community health center system is a $7 billion annual revenue hole that a rural health program does not fill.
A bandage on a Medicaid wound does not close the wound. It makes the press release look better.
The CFOs, medical directors, and board chairs running community health centers deserve more than a headline. They deserve a policy environment that takes their financial model seriously - and they deserve health system leaders, investors, and advocates who understand the sequence before the closures start.
What is your December 2026 contingency plan?
About the Author
Jonathan Govette is the Co-Founder and CEO of Oatmeal Health, an AI lung cancer diagnostic company catching cancers earlier in the communities that need it most. Oatmeal uses AI to identify unscreened high-risk patients, navigate them to care, and score every lung CT for malignancy risk - billed under CPT 0721T. Stage I survival is 77%. Stage IV is 9%. We work in FQHCs because that gap is largest there.
Jonathan writes daily about radiology, pulmonology, AI diagnostics, health policy, hospital operations, and healthcare startups.
Subscribe to stay ahead of healthcare's most important shifts. Weekly deep-dives on AI, radiology, health policy, FQHCs, and the business of healthcare - written for operators, clinicians, and investors who want the signal, not the noise. Subscribe at oatmealhealthjonathangovette.substack.com
Key References
NACHC: Proposed Changes in Reconciliation Bill Jeopardizes Care for Community Health Center Patients Insured through Medicaid (nachc.org)
CMS: CMS Announces $50 Billion in Awards to Strengthen Rural Health in All 50 States (cms.gov)
KFF: Community Health Center Patients, Financing, and Services - Impact of Federal Policy Changes (kff.org)
STAT News: The greatest threat to federally qualified health centers may not be federal funding cuts (statnews.com, March 2026)
Advocates for Community Health: Special Report - The Critical Role of 340B at FQHCs (advocatesforcommunityhealth.org)