

Cadence: AI Agents for Chronic Care
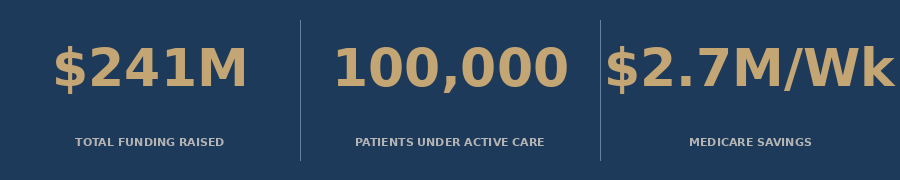
A $241M startup just proved AI agents can manage 100,000 chronic disease patients at scale - and Medicare saves $2.7 million every week because of it.


Every care manager in America is running the same impossible math.
More patients. Fewer clinicians. Chronic conditions that demand daily attention but receive monthly appointments. Heart failure that decompensates between visits. Hypertension that goes uncontrolled because no one is watching between the third Tuesday of every month.
This is not a staffing problem. It is a contact frequency problem.
And Cadence just raised $100 million to fix it.
On June 23, 2026, Cadence announced a Series C led by Spark Capital, bringing total funding to $241 million at a $1.23 billion valuation. The round included Thrive Capital, General Catalyst, Coatue, B Capital, and the venture arms of Corewell Health, Memorial Hermann, and Duke Health.
The company is treating 100,000 patients today with AI agents that monitor their chronic disease in real time. And it tripled annual recurring revenue in 2025.
Here is what the funding announcement obscures: this is not a remote monitoring company. Cadence is an AI-operated chronic care delivery system. That distinction is the entire business model.
1. The Chronic Disease Crisis Is a Contact Problem
56 million older adults in the United States live with at least one chronic condition requiring active management. The real number is higher: between 55 and 98 percent of adults over 60 have two or more chronic diseases simultaneously.
Heart failure affects 7.7 million Americans, up from 6.7 million just three years ago. It is the fastest-growing cardiovascular phenotype in the country. Hypertension and diabetes co-occur in more than one-third of all Medicare beneficiaries. Nearly half of US adults now meet criteria for cardiovascular disease when hypertension is included.
The clinical consequence of this is straightforward: these patients need more contact points than the current system provides.
A physician managing a heart failure patient on four guideline-directed therapies cannot clinically monitor them adequately in a 15-minute quarterly appointment. Blood pressure does not cooperate with scheduling. Medication adherence does not pause for office hours. Fluid accumulation does not announce itself with enough warning for a monthly check-in to catch it in time.
📊 The average heart failure patient is hospitalized 1.3 times per year. Each admission costs the system approximately $21,000. At 7.7 million patients, that is a $198 billion annual inpatient cost line driven in large part by preventable decompensation.
The care model is not working because the contact model is broken.
Traditional chronic care management - in-person visits, monthly calls, quarterly labs - was designed for an era when chronic conditions were exceptions, not the rule. When 55 to 98 percent of your patients have multiple conditions, monthly touch points are not care management. They are triage intervals.
2. What Cadence Actually Builds
Cadence is not a monitoring company. Most remote patient monitoring companies give clinicians a dashboard - more data, more alerts, more things to triage. That is adding cognitive burden to a workforce already at capacity.
Cadence built the layer between the sensor and the clinician.
Patients are enrolled with connected devices that track vitals continuously. AI agents monitor that data stream, apply risk stratification models, surface alerts that need attention, and in 55 percent of cases resolve those alerts without requiring any human clinical time at all. When the AI flags something that warrants a human touch, the median response time for a care team member is 3.5 minutes.
The AI agents handle the routine. The clinicians handle the irreplaceable.
This matters because the math of traditional CCM breaks down at scale. A single care manager can meaningfully manage somewhere between 80 and 120 patients under traditional workflows. With AI handling triage, alert resolution, and documentation, that ratio changes dramatically.

Cadence charges payers - primarily Medicare - a monthly per-patient fee for this service. The company operates as a clinical service business, not a technology licensing company. It takes accountability for outcomes, not just data delivery.
New affiliations with Duke Health and Texas Health Resources, both announced alongside the Series C, expand the network of health systems using Cadence as a chronic care delivery layer. These are not pilot agreements. They represent full deployment at health systems that collectively serve hundreds of thousands of Medicare patients.
3. The Outcomes That Actually Matter
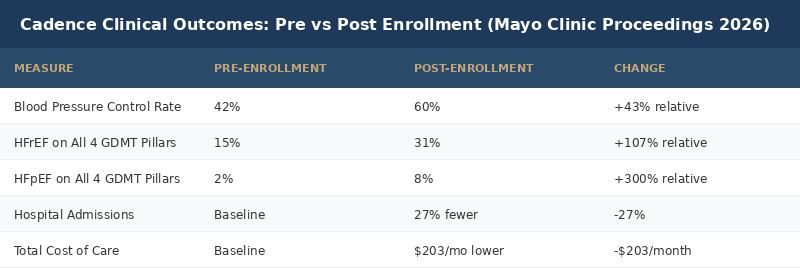
In February 2026, Cadence published results in Mayo Clinic Proceedings: Innovations, Quality and Outcomes. The study, titled "The Impact of a Remote Patient Care Program on Health Care Costs and Utilization Among Medicare Patients With Chronic Disease," is the most rigorous validation of their model to date.
The numbers are not incremental.
Blood pressure control improved by 43 percent relative to baseline - from 42 percent of patients controlled to 60 percent. Systolic blood pressure fell by 6.9 mmHg. Diastolic by 4.9 mmHg. Both statistically significant.
In heart failure patients with reduced ejection fraction, the percentage on all four guideline-directed medical therapy pillars doubled - from 15 percent to 31 percent. That is a 107 percent increase in appropriate GDMT adherence. In patients with preserved ejection fraction, the improvement was even more dramatic: from 2 percent to 8 percent, a 300 percent relative increase.
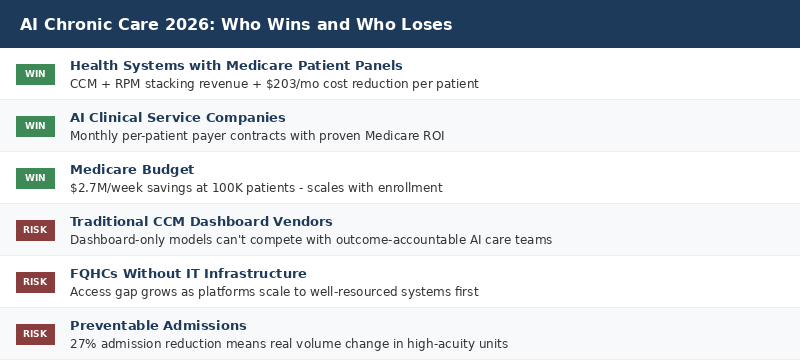
Hospital admissions fell 27 percent.
Total cost of care fell by $203 per patient per month.
📊 At 100,000 active patients, that $203/month cost reduction translates to more than $243 million in annual system savings - and Cadence is saving Medicare $2.7 million every single week.
These outcomes are not from a controlled academic trial with cherry-picked patients. This is real-world Medicare data across a diverse patient population, including rural and underserved communities.
That last detail matters. Clinical trials that exclude low-income and minority patients have historically produced results that do not hold up in the populations where chronic disease burden is highest. Cadence's outcomes data holds in those populations.
4. The Reimbursement Architecture Underneath This
The financial model of AI-powered chronic care is not complicated, but most health systems do not have a team that has mapped it.
Medicare has an established billing framework for chronic care management and remote patient monitoring. The 2026 Medicare Physician Fee Schedule increased CCM reimbursement by 10 percent across all codes - the largest single-year increase in program history. Two new RPM codes were added: CPT 99445 for 2-15 days of monitoring data and CPT 99470 for the first 10 minutes of monitoring time.
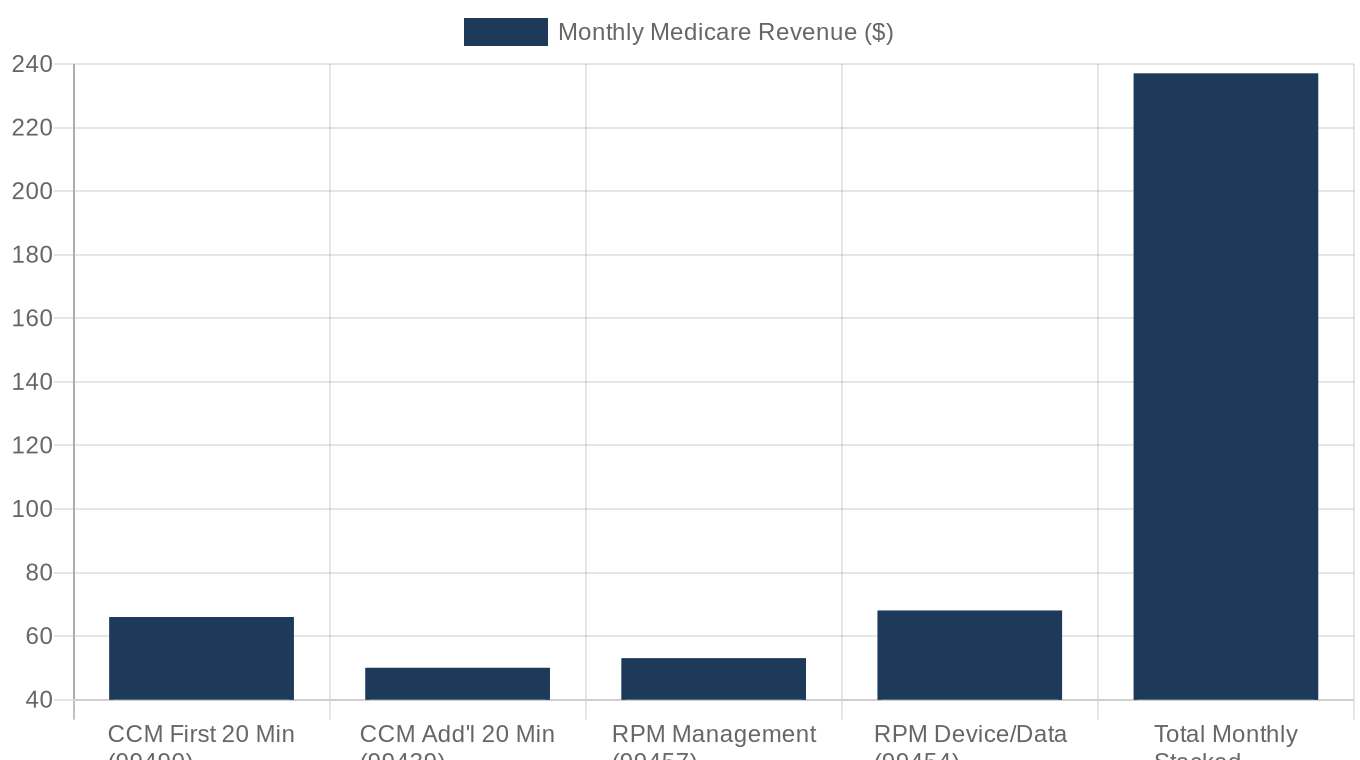
The revenue architecture, stacking CCM and RPM together, looks like this:
CPT 99490: $66.13 per patient per month (first 20 minutes of non-complex CCM)
CPT 99439: ~$50.44 per patient per month (additional 20 minutes)
CPT 99457: ~$53 per patient per month (first 20 minutes RPM management time)
CPT 99454: ~$68 per patient per month (device supply and data transmission)
Layered appropriately, CCM plus RPM generates approximately $200 to $300+ per patient per month in Medicare reimbursement.
This is not speculative revenue. This is Medicare reimbursement at established rates. The constraint has never been the billing codes. It has been the clinical capacity to actually deliver the required monitoring and management time. That is exactly what AI agents address.
5. The FQHC Opportunity - and the Gap That Still Exists
Federally Qualified Health Centers are the natural home for this model.
The patient populations FQHCs serve - low-income adults, uninsured and Medicaid-dependent households, rural communities with limited specialist access - carry the highest chronic disease burden in the country. Hypertension, diabetes, heart failure, and COPD concentrate in the same zip codes that FQHCs serve. These patients have the most to gain from continuous monitoring and the least access to the traditional care model.
And yet, FQHC adoption of RPM and AI-assisted chronic care management remains low.
The barriers are real. Broadband access is inconsistent in the communities FQHCs serve. Not all patients have smartphones with reliable data plans. Device procurement requires upfront capital that community health centers on 55 percent cost-to-revenue ratios cannot easily absorb. And the IT staffing to implement, configure, and troubleshoot a remote monitoring program typically does not exist at a center running one IT staffer across ten sites.
📊 A 2026 survey of FQHC administrators found that more than 60 percent cite lack of dedicated care management staff as the primary barrier to scaling RPM programs - not reimbursement, not patient willingness.
The 2026 CMS rule changes help at the margin. The new CPT 99445 code - which allows billing for 2-15 days of monitoring data instead of requiring a full 16 days - reduces the program enrollment burden significantly for patients who cannot maintain daily device contact.
But the structural access problem for FQHCs goes deeper than billing codes.
A model like Cadence's, where AI agents handle the monitoring workload and human clinical time is deployed only for cases that require it, is specifically designed to address the FQHC staffing constraint. The question is whether health systems and FQHCs can establish partnership arrangements that give safety-net providers access to the platform economics that currently flow primarily to large health systems with existing revenue cycle infrastructure.
6. The Competitive Landscape
Cadence is not operating in an empty market.
Biofourmis, which has raised more than $463 million in total funding, targets the same space with a focus on wearable biometric sensors and predictive deterioration models, particularly for cardiovascular and respiratory conditions. Innovaccer has positioned itself as a data platform play, integrating disparate health records and layering care management analytics on top.
What distinguishes Cadence is the clinical service model rather than the technology licensing model. Cadence does not sell a platform and walk away. It operates as a care team member, taking accountability for outcomes and billing Medicare directly. That accountability alignment - where the company's revenue depends on keeping patients healthy and out of the hospital - is what justifies the clinical confidence to report Mayo Clinic outcomes publicly.
The AI in remote patient monitoring market is valued at $3.35 billion in 2026 and is projected to grow at a 27 percent CAGR through 2031. With Cadence at $1.23 billion valuation, it is one of the most valuable standalone players in a market that is still early in consolidation.
Deep Dive: The Unit Economics of AI-Managed Chronic Care
The $100 million Series C is a bet on a specific unit economics model, and the math is worth understanding in detail.
Cadence is treating 100,000 patients today. Its Mayo Clinic Proceedings data shows $203 per patient per month in total cost-of-care reduction. At current enrollment, that is approximately $20.3 million per month, or $243.6 million per year, in system savings.
Medicare pays for the care management through CCM and RPM codes. Stacked appropriately, a patient enrolled in a comprehensive program generates approximately $200 to $300 per patient per month in billable services.
Cadence takes a service fee from health systems or payers. The company has published that it delivers "more than $3 in Medicare savings for every dollar Medicare spends." At $200 per patient per month in reimbursement and $600+ in savings, the ROI justification for a payer or health system to contract with Cadence is not abstract.
The visual below breaks out the annual value per patient across the four components of the Cadence economic model.
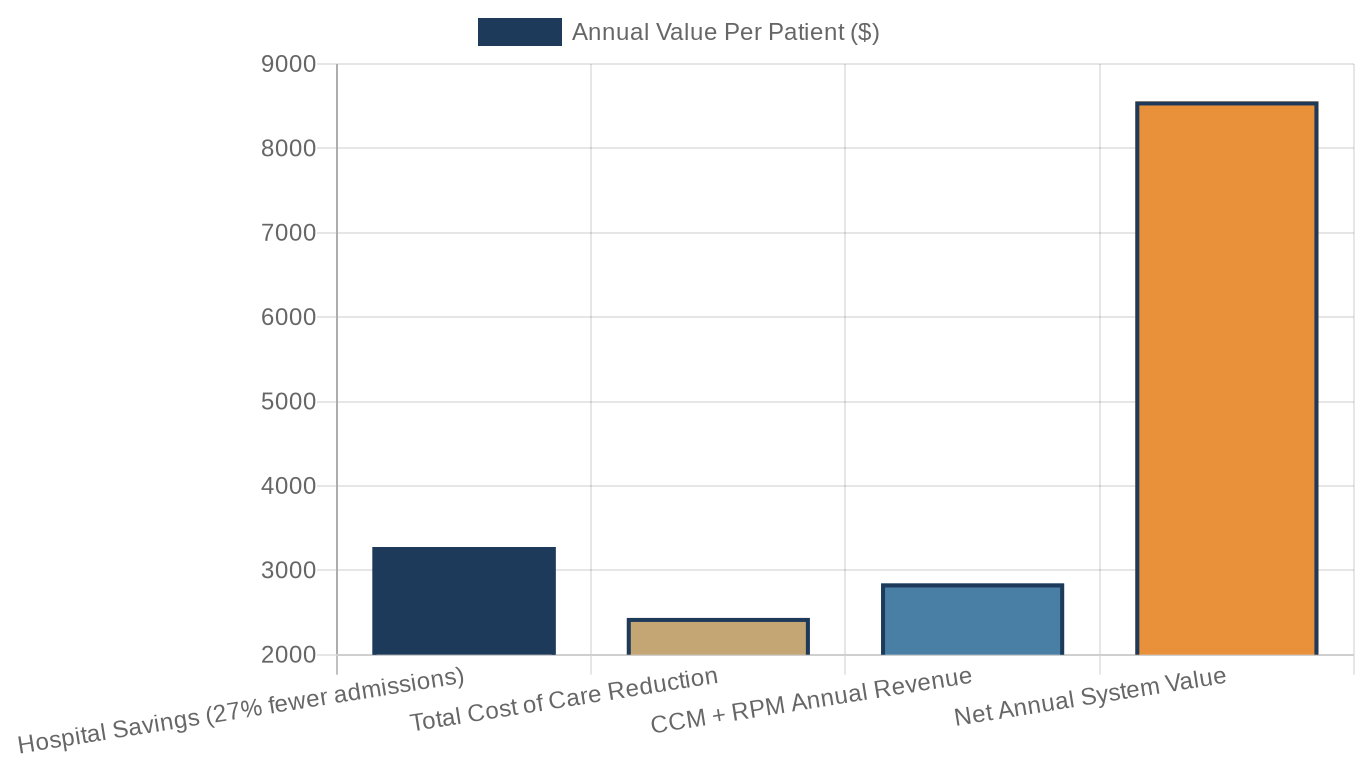
The Scale Trajectory
Cadence tripled annual recurring revenue in 2025. The Series C is designed to accelerate the next growth phase: deeper health system partnerships, expansion into new chronic conditions beyond hypertension and heart failure, and geographic expansion into markets where chronic disease burden is highest.
The Duke Health and Texas Health Resources affiliations signal the kind of institutional validation that drives payer adoption. When an academic medical center puts its name on a partnership, it signals clinical confidence that accelerates commercial contracting.
The Risk Factors
The model's strength is also its primary risk. Cadence takes accountability for outcomes. If outcomes degrade at scale - if the clinical quality that produced those Mayo Clinic Proceedings numbers does not hold across 500,000 patients - the revenue model unwinds.
The AI agent layer is not infinitely scalable without ongoing model validation. Alert fatigue, false negative suppression, and model drift are real risks in any AI clinical system. At 55 percent of alerts resolved by AI without human review, the quality of that automated resolution layer is load-bearing for patient safety.
The second risk is payer negotiations. Medicare reimbursement rates are not guaranteed to stay at 2026 levels. Any downward fee schedule adjustment to CCM or RPM codes directly compresses Cadence's unit economics.
What This Means For You
FQHC executives and community health center CEOs: The Cadence model is designed to address your staffing constraint - AI agents handling triage so your limited clinical staff handle only cases that require human judgment. The barrier is partnership access and IT infrastructure, not patient eligibility. Push your health system partners on whether chronic care AI platforms can extend to your patient panel under their contracts.
Health system CMOs and CFOs: At $203 per patient per month in cost reduction and $200 to $300 in stacked CCM/RPM reimbursement, the ROI math on AI-assisted chronic care is not ambiguous. The question is not whether to deploy this model - it is whether to build, partner, or acquire your way into it before your competitor does.
Radiologists and pulmonologists: Your highest-acuity lung and cardiac patients are often the same patients with uncontrolled chronic disease at the time of diagnosis. AI chronic care management that achieves guideline-directed therapy compliance before a cancer or cardiac event improves the outcomes you are measuring at the time of intervention.
Healthcare investors and founders: The AI in RPM market is valued at $3.35 billion in 2026 with a 27 percent projected CAGR. Clinical service models with accountable outcome contracts are outcompeting pure technology licensing models. Follow the payer contract structure, not the software pitch.
Policy advocates: The Cadence model saves Medicare $2.7 million every week at 100,000 patients. Scaling this to the millions of eligible Medicare beneficiaries who currently receive inadequate chronic care management would generate billions in program savings annually. CMS should be examining how to accelerate this model in safety-net settings, not just at large health systems with existing infrastructure.
The future of chronic care is not more clinicians. The country cannot train them fast enough. It is not more monitoring dashboards. Those already exist and are already being ignored.
The future of chronic care is AI agents that handle the contact frequency problem automatically, surface only the cases that require human judgment, and give clinicians back the time to do the work that actually requires them.
Cadence just proved that model works at scale. And Medicare is paying for it.
The question for every health system CEO reading this: what is your chronic care management strategy, and does it account for a world where your competitors' AI agents are monitoring 100,000 patients while yours are reading dashboards?
Reply to this email with your answer. I read everything.
About the Author
Jonathan Govette is the Co-Founder and CEO of Oatmeal Health, an AI lung cancer diagnostic company catching cancers earlier in the communities that need it most. Oatmeal uses AI to identify unscreened high-risk patients, navigate them to care, and score every lung CT for malignancy risk - billed under CPT 0721T. Stage I survival is 77%. Stage IV is 9%. We work in FQHCs because that gap is largest there.
Jonathan writes daily about radiology, pulmonology, AI diagnostics, health policy, hospital operations, and healthcare startups.
Subscribe to stay ahead of healthcare's most important shifts. Weekly deep-dives on AI, radiology, health policy, FQHCs, and the business of healthcare - written for operators, clinicians, and investors who want the signal, not the noise. Subscribe at oatmealhealthjonathangovette.substack.com
Key References
Cadence $100M Series C announcement (Business Wire, June 23, 2026)
Mayo Clinic Proceedings: "The Impact of a Remote Patient Care Program on Health Care Costs and Utilization Among Medicare Patients With Chronic Disease" (February 2026)
2026 CCM/RPM Reimbursement Rates: CPT 99490 at $66.13/month; 10% CCM increase across all codes (CMS 2026 PFS Final Rule)
AI in Remote Patient Monitoring Market (MarketsandMarkets, 2026): $3.35B market, 27% CAGR through 2031
FQHCs and RPM in 2026: Barriers and CMS Policy Changes (Prevounce, Tenovi, 2026)