

AI Radiology: Speed vs. Accuracy Tradeoff
ECRI ranked over-reliance on AI the No. 1 patient safety threat of 2026. The question is not whether AI makes radiology faster - it is whether faster is actually safer.


AI is reading chest X-rays faster than ever before.
Aidoc's January 2026 FDA clearance covers 14 conditions at 97% mean sensitivity and 98% mean specificity. AI triage tools are prioritizing worklists in real time, flagging critical findings in seconds, and promising to close the widening gap between imaging volume and radiologist capacity. The vendor dashboards look impressive. The benchmark numbers look convincing.
But in March 2026, the patient safety organization ECRI published its annual watch list and named "Navigating the AI diagnostic dilemma" as healthcare's single biggest patient safety risk of the year. Not data breaches. Not medication errors. AI diagnosis.
That is not a coincidence. That is a warning the field has not fully absorbed.

1. The Automation Bias Problem Nobody Wants to Name
Automation bias is not a theoretical risk. It has been documented across aviation, nuclear operations, and now, repeatedly, in clinical radiology.
The concept is straightforward: when a human works alongside an automated system, they unconsciously defer to the machine's output, especially under cognitive load. When the AI clears a scan, the radiologist reviews it less carefully. When the AI flags something urgent, they scrutinize it more. The AI shapes attention - even when the AI is wrong.
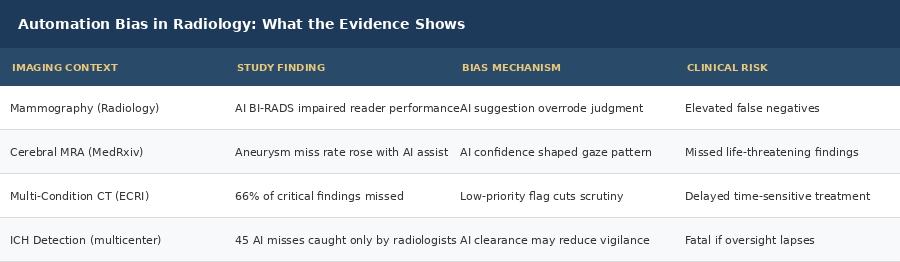
A peer-reviewed study published in Radiology found that incorrect advice from a purported AI decision support system measurably impaired radiologist performance across experience levels. The more trusted the AI appeared, the larger the impairment.
A separate study on cerebral aneurysm detection via time-of-flight MRA confirmed the same pattern. Radiologists working with AI assistance showed automation bias in a high-sensitivity imaging context. The AI's confidence score shaped where radiologists looked - and what they missed.
This is not a technology failure. It is a human-machine interaction problem that no accuracy benchmark on a vendor slide captures.

The fundamental issue with how most radiology AI is deployed today: vendors measure sensitivity and specificity on curated benchmark datasets. They do not measure how radiologist behavior changes after the AI makes a call. That behavioral shift is where diagnostic risk accumulates in production.
When an AI system marks 80% of scans as low priority, what happens to radiologist attention on case 73 in a 90-case worklist? That question does not appear in any sensitivity curve. But the answer matters more than the benchmark.
2. What ECRI's Warning Actually Means
ECRI's 2026 report is not speculative. It is grounded in documented failure patterns across actual clinical deployments.
Some machine learning models tested in simulated diagnostic scenarios failed to recognize 66% of critical or deteriorating health conditions. Not rare edge cases. Common presentations that a competent clinician would flag immediately.
When AI misses a critical finding, it does not return an error message. It returns a low-priority designation. A confident-sounding negative. That is the mechanism through which automation bias causes patient harm: not a software crash, but a subtle signal that reassures when it should not.
The specific failure modes ECRI identified include rare diseases and uncommon presentations, subtle early-stage findings in complex anatomies, and cases where imaging alone cannot tell the full story without clinical context. These are precisely the cases where a careful radiologist would ordinarily spend more time. When AI assigns them a low-priority flag, that extra time evaporates.
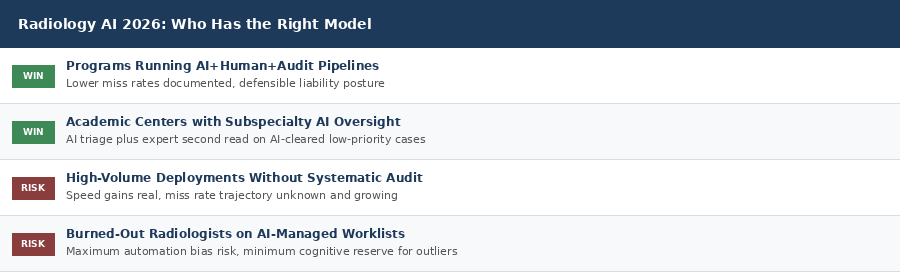
Radiology is also facing a structural workforce crisis that makes this worse. Practice turnover among radiologists increased 61% between 2013 and 2022, and radiologists are leaving practice entirely at more than twice the rate of a decade ago. Burnout affects 46% of private practice radiologists and 37.4% in academic settings. A burned-out radiologist reviewing AI-flagged worklists at the end of a high-volume shift is the exact profile most susceptible to automation bias.
3. The Accountability Gap at the Heart of AI Radiology
One of the starkest blind spots in how health systems are deploying radiology AI: almost no organizations are auditing AI-assisted reads against gold-standard re-reads at scale.
Vendors report benchmark accuracy. Health systems report turnaround time reduction. What almost no one is reporting is the false negative rate stratified by AI confidence score - the one metric that would directly reveal automation bias in their own deployment.
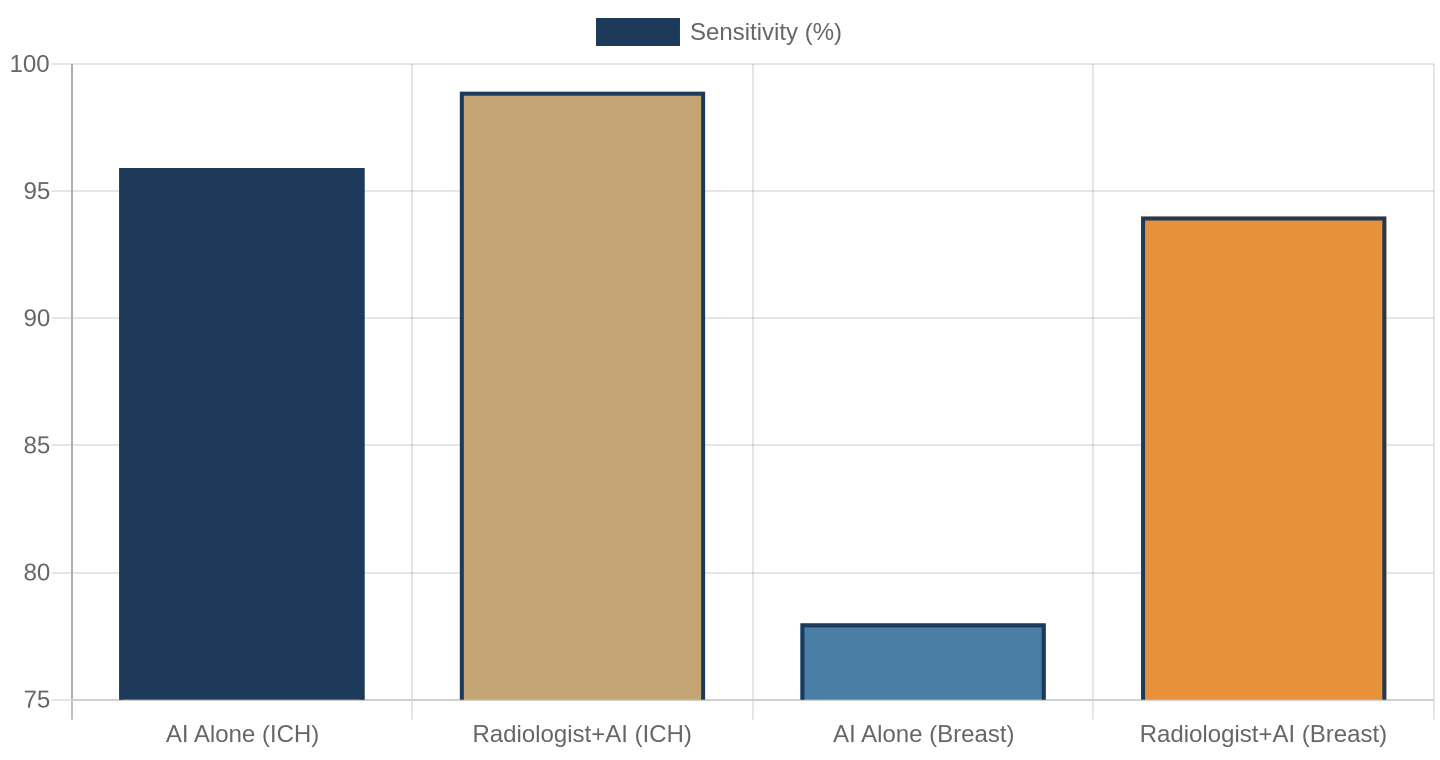
A 2025 prospective multicenter study on AI-assisted intracerebral hemorrhage detection found that AI-assisted radiologists achieved 98.91% sensitivity compared to 95.91% for AI alone. The critical finding: all 45 cases missed by AI were caught by radiologists, and all 12 cases missed by radiologists were caught by AI. Human and AI failures are complementary but do not overlap. An AI clearance that reduces radiologist scrutiny on a case the AI missed is exactly where harm concentrates.
The accountability gap has three dimensions most health systems are not addressing. First, liability: most radiology AI vendor contracts place responsibility for diagnostic errors on the signing radiologist, not the AI tool. Second, governance: CMS and the Joint Commission have not issued formal guidance on AI-assisted diagnostic reads, leaving most health systems writing their own policies with wildly varying quality. Third, operations: worklist design that routes radiologists to AI-flagged cases first and AI-cleared cases last means fatigue accumulates exactly where caution is most needed.
4. What the Data Actually Shows
The picture from peer-reviewed research in 2025 and 2026 is more nuanced than the vendor pitch or the automation bias critique alone would suggest.
In well-defined, high-volume applications, AI-assisted accuracy data is genuinely impressive. Breast cancer AI flagged 49.8% of interval cancers missed by human readers. AI decreased false positives by 37.3% and reduced unnecessary biopsies by 27.8% in breast imaging programs. For rib fracture detection, AI achieved a median inference time of 10.6 seconds versus 3.3 hours for human reports, with no compromise in accuracy on that specific task.
The challenge is that radiology is not a single well-defined task. It is hundreds of different diagnostic problems distributed across imaging modalities, patient populations, and disease stages. An AI that achieves 98% sensitivity on PE detection in a controlled trial may perform meaningfully differently when deployed across the heterogeneous scan volume of a community hospital.
A 2026 systematic review of AI generalizability found that performance metrics from controlled trials frequently do not replicate when the same tools are deployed in different clinical settings, patient populations, or imaging acquisition protocols. The gap between benchmark and real-world performance is not a bug. It is a structural feature of how AI is trained and how clinical settings vary.
Speed improvements are real. Accuracy improvements are conditional. The conditions are site-specific and modality-specific. That complexity is not reflected in how most health systems make AI procurement decisions today.
5. The Missing Metric: AI Confidence vs. Miss Rate
Here is the specific audit that most radiology AI deployments are not running, and should be.
Track the false negative rate stratified by AI confidence score. For cases where the AI assigned a low-priority or negative classification, what percentage contained a significant finding that was later identified? And how does that rate change as radiologist case volume increases across a shift?
This metric directly reveals automation bias in a live deployment. It is not complicated to generate. It requires structured re-reads of a sample of AI-cleared cases combined with outcome tracking. The information exists in most health systems' PACS and RIS systems. It is simply not being extracted and analyzed.
The most forward-thinking radiology programs in 2026 are running exactly this kind of audit. They are tracking miss rates by AI confidence bucket, measuring whether low-priority cases generate proportionally more subsequent imaging orders or escalations than the AI flag suggested, and using that data to calibrate how aggressively the AI's low-priority designations influence worklist positioning.
The math is not close. A quarterly audit of 200 randomly sampled AI-cleared cases costs roughly $10,000 to $40,000 in re-read labor at current rates. The avoided liability exposure from a single missed lung cancer diagnosis in most U.S. jurisdictions exceeds $1 million. The audit program pays for itself on the first miss it prevents.
6. The Regulatory Landscape Has Not Caught Up
The FDA has cleared more than 1,524 AI-enabled radiology devices as of mid-2026. The pace of clearances is accelerating: 68 new algorithms in the first quarter of 2026 alone. Breakthrough Device Designations are now being granted to generative AI systems that draft entire radiology reports, not just flag findings.
The governance infrastructure has not kept pace.
Current FDA clearance processes evaluate algorithm performance on training and test datasets. They do not require pre-market demonstration of real-world performance in heterogeneous clinical settings, post-deployment monitoring of false negative rates stratified by AI confidence, or vendor notification when site-specific performance drifts below benchmark thresholds.
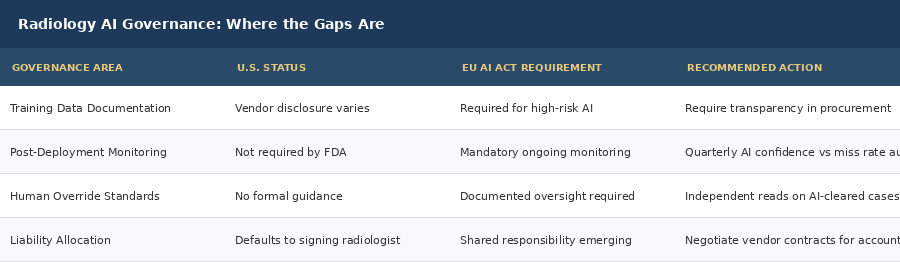
The EU AI Act, fully effective in 2026, requires that high-risk AI systems including AI in medical diagnosis document training data curation, bias checks, and human oversight policies. European health systems deploying radiology AI are building those governance frameworks now. Most U.S. health systems are not.
The liability landscape is also evolving. Malpractice attorneys are actively building cases around the radiologist-as-rubber-stamp scenario: a radiologist who signed an AI-generated read without meaningful independent review on a case where the AI missed a significant finding. This is not hypothetical. The case law is beginning to accumulate.
Deep Dive: The Real Cost of an Unaudited Deployment
Let me walk through the math of what an unaudited AI radiology deployment actually costs when automation bias generates a missed finding.
In the best-case scenario, an AI system performing at 97% sensitivity on its benchmark dataset misses 3% of positive cases. In a high-volume setting reading 10,000 scans per month, that is 300 cases per month where a positive finding was not flagged by the AI. If automation bias causes radiologists to review AI-cleared cases with 20% less scrutiny - a conservative estimate from the automation bias literature - the proportion of those 300 cases that also get missed by the radiologist increases meaningfully.
Scenario A: High-Volume Site, No Audit Program
Reading 10,000 chest CTs per month. AI benchmark sensitivity: 97%. Real-world sensitivity estimate given distribution shift: 94%. Cases with positive findings: assume 15% of volume, or 1,500 cases. AI misses 6% of those: 90 cases per month with positive findings cleared as low priority. Automation bias increases miss rate on those cases by an estimated 20% relative to normal scrutiny. Result: roughly 18 additional missed findings per month introduced by unmonitored AI workflows. Annualized: over 200 missed findings per year that a properly governed deployment would catch.
Scenario B: Same Site, With a Quarterly Audit Program
Same scan volume. Same AI. But quarterly audit of 200 randomly sampled AI-cleared cases against a radiologist re-read. Miss rates are measured, reported, and used to adjust worklist protocols. Radiologists are briefed on their AI-assisted miss rate trends each quarter. Result: automation bias is detected and quantified within 90 days. Protocol adjustment alone cuts miss rates by an estimated 40-60%. Additional cost: roughly 800 re-reads per year. Avoided liability exposure from a single missed lung cancer diagnosis: well above $1 million in most U.S. jurisdictions.
The math is not close. The audit program pays for itself on the first miss it prevents.
What This Means For You
For FQHC executives and community health center leaders: if you are evaluating or using AI-assisted diagnostic imaging tools, ask every vendor for their false negative rate on cases they assigned low priority. If they cannot produce that number, that is your answer.
For health system administrators and CMOs: build the audit layer before expanding AI deployment. Measuring turnaround time without measuring miss rates is measuring the wrong thing. Implement structured re-read protocols for a random sample of AI-cleared low-priority cases quarterly.
For radiologists and radiology department chiefs: the legal exposure is yours. Until contract terms shift accountability to AI vendors, your defense against a missed finding claim depends on documentation that you conducted a meaningful independent review. Know your institution's protocol for AI-assisted reads.
For healthcare investors and founders: governance and audit infrastructure is the competitive moat in radiology AI that nobody has built yet. The first platform that provides site-specific AI confidence versus miss rate dashboards will be the one health systems lock into long-term.
For policy advocates: push CMS and the FDA to require post-deployment performance monitoring as a condition of continued AI clearance in radiology. The EU model is available to adapt.
Closing
The radiology AI story of 2026 is not one of failure. It is one of an industry moving faster than its own accountability infrastructure can follow.
AI tools that triage worklists, flag critical findings, and assist with structured reporting are genuinely valuable. The data on their performance in well-matched applications is real. The case for deploying them is not in question.
What is in question is whether health systems are building the oversight layer that makes AI-assisted radiology safer than unassisted radiology, not just faster.
ECRI did not name AI diagnosis the No. 1 patient safety risk of 2026 because AI does not work. They named it because AI works well enough that clinicians stop checking.
Speed without oversight is not an upgrade. It is a liability dressed as a solution.
The question worth asking in every radiology department reading this: do you know your AI-assisted miss rate on cases the algorithm cleared? If not, that is the most important metric your team is not yet measuring.
Jonathan Govette is the Co-Founder and CEO of Oatmeal Health, an AI lung cancer diagnostic company catching cancers earlier in the communities that need it most. Oatmeal uses AI to identify unscreened high-risk patients, navigate them to care, and score every lung CT for malignancy risk - billed under CPT 0721T. Stage I survival is 77%. Stage IV is 9%. We work in FQHCs because that gap is largest there.
Jonathan writes daily about radiology, pulmonology, AI diagnostics, health policy, hospital operations, and healthcare startups.
Subscribe to stay ahead of healthcare's most important shifts. Weekly deep-dives on AI, radiology, health policy, FQHCs, and the business of healthcare - written for operators, clinicians, and investors who want the signal, not the noise.
Subscribe at oatmealhealthjonathangovette.substack.com
Key References
ECRI 2026 Patient Safety Watch: "Navigating the AI Diagnostic Dilemma" - ranked No. 1 patient safety concern for 2026.
Radiology (RSNA): Automation bias study on AI-assisted mammography - incorrect AI suggestions impaired radiologist performance across experience levels.
Neiman Health Policy Institute: Radiologist practice turnover increased 61% between 2013 and 2022; radiologists leaving practice at twice the rate of a decade ago.
Prospective multicenter ICH study 2025: AI-assisted radiologists at 98.91% sensitivity vs. 95.91% for AI alone; all 45 AI misses were caught by radiologists.
ECRI 2026: Some ML models failed to recognize 66% of critical conditions in simulated cases.