

AI Health Startup Raises $100M+
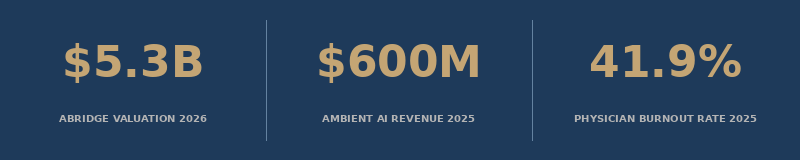
Abridge just crossed a $5.3 billion valuation. Ambient AI documentation is healthcare's first proven AI category at scale. But the question no one is asking is whether we are fixing the right problem.

In February 2025, Abridge raised $250 million in a Series D round, bringing its valuation to $2.75 billion. That was a signal.
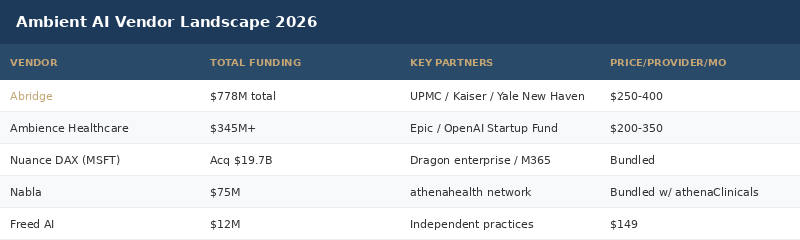
Four months later, Andreessen Horowitz led a $300 million Series E, pushing the valuation to $5.3 billion. Then in April 2026, Abridge raised another $316 million extension. Total capital raised: $778 million.
That is not a bet on future potential. That is a bet on a proven category.
Ambient AI clinical documentation - the technology that listens to physician-patient conversations and automatically generates clinical notes in the EHR - has become healthcare AI's first genuine breakout business. The category generated $600 million in revenue in 2025, a 2.4x year-over-year jump. The global ambient intelligence market sits at $37.2 billion today and is projected to cross $91 billion by 2030.
Investors are not funding ambient AI because the products are impressive. They are funding it because the problem it solves is real, measurable, and expensive in ways that spreadsheets can actually capture.
The problem is physician burnout. The Stanford estimate: $4.6 billion per year in costs to the U.S. healthcare system from burnout-related turnover, reduced productivity, and care quality degradation. Clinicians spend, on average, nearly two hours on EHR tasks for every one hour of direct patient care. Specialties with the highest documentation burden - family medicine, internal medicine, emergency medicine - report the worst burnout rates.
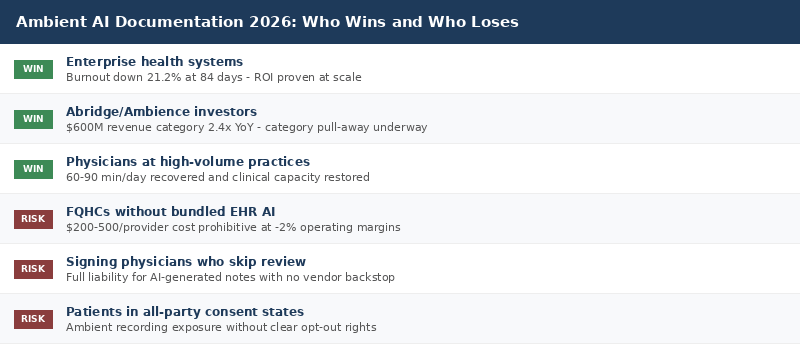
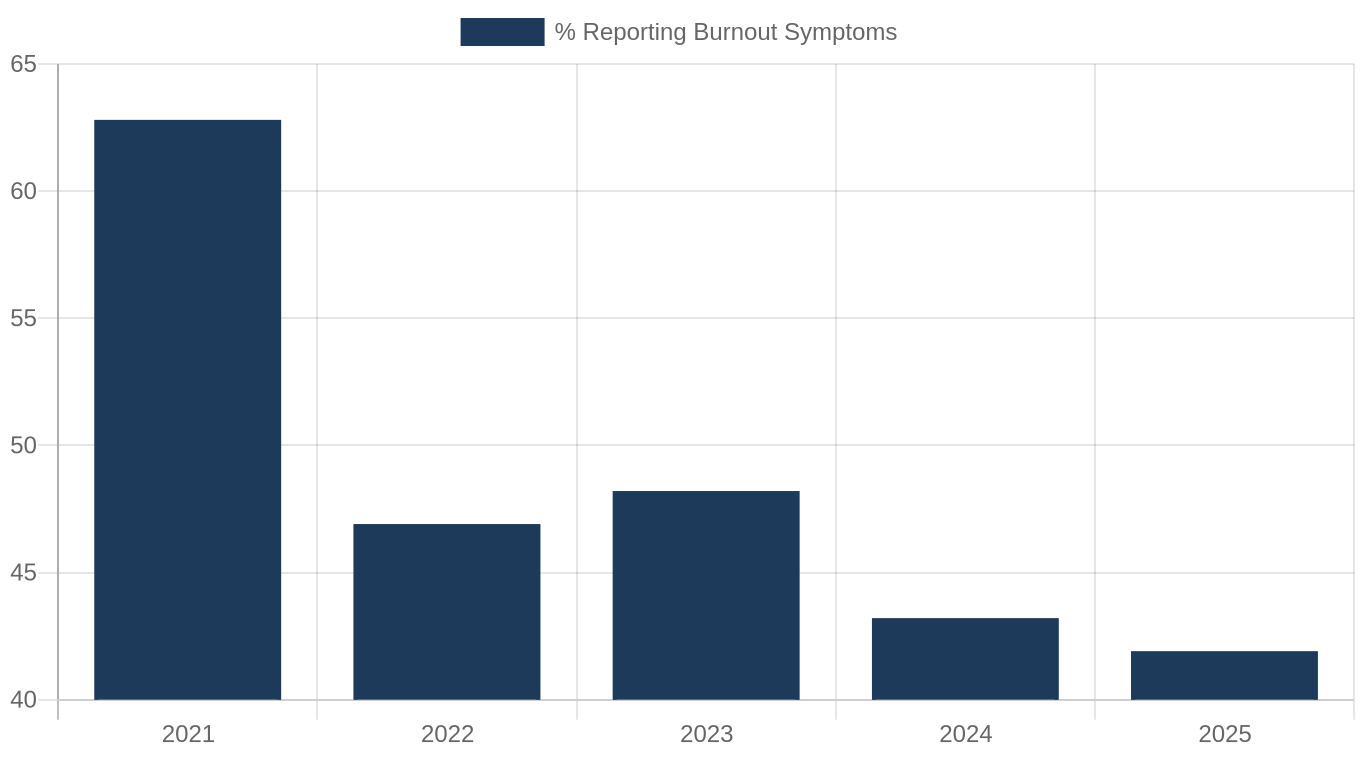
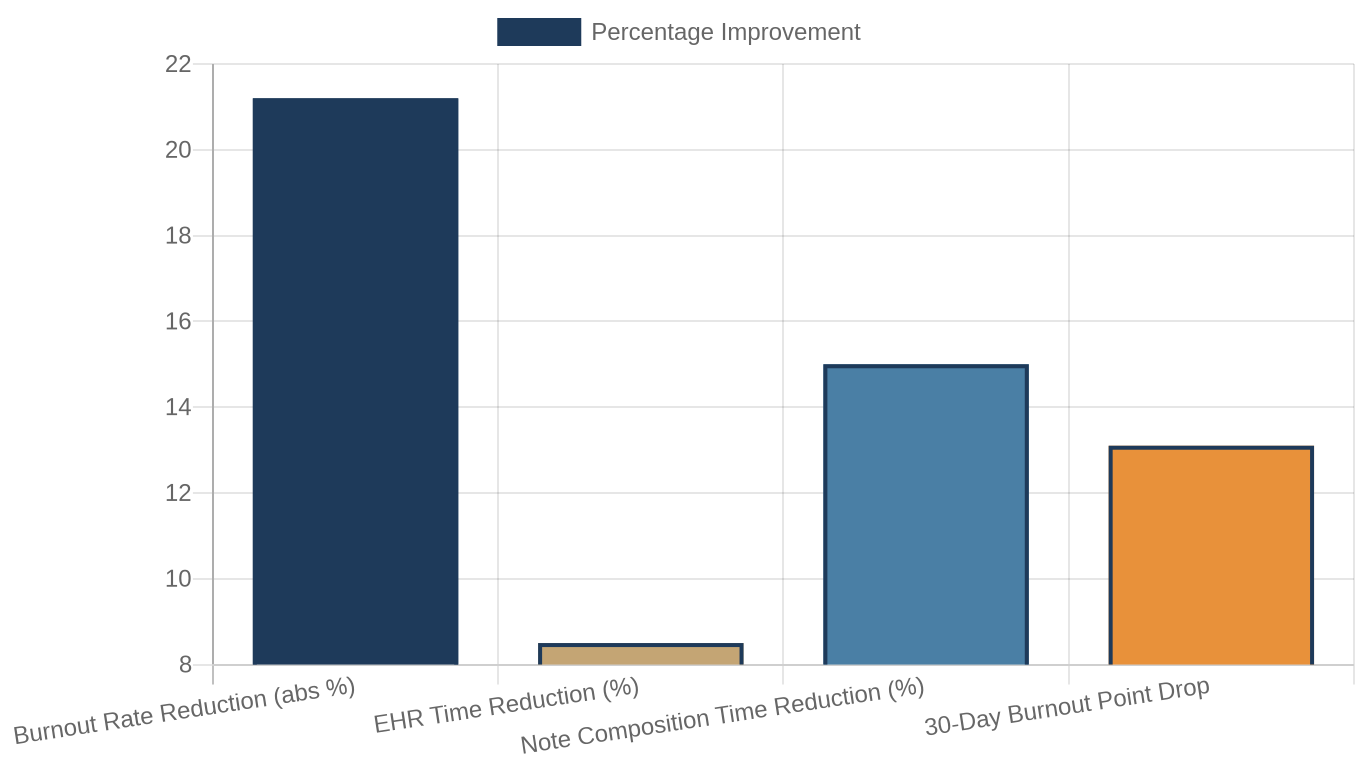
Ambient AI attacks that ratio. And for the first time in years, the data shows it is working. Burnout rates among physicians have dropped four consecutive years, from 62.8% in 2021 to 41.9% in 2025. Studies at Mass General Brigham showed a 21.2% absolute reduction in burnout prevalence at 84 days of ambient AI use. Clinicians spent 8.5% less total time in the EHR and 15% less time composing notes.
These are not pilot numbers from a curated cohort. These are real health system results. The technology works.
But there is a harder question underneath the funding headlines.
1. What Ambient AI Actually Fixes - and What It Does Not

Ambient AI does exactly what it promises. It listens. It structures. It generates. A physician walks out of an exam room with a note already drafted in the EHR. No after-hours charting. No pajama time. The technology has matured from clunky speech-to-text into contextually sophisticated clinical documentation that understands SOAP structure, ICD-10 coding context, and specialty-specific terminology.
Two-thirds of U.S. hospitals using Epic's EHR had adopted ambient AI tools as of June 2025. That is not a niche adoption curve. That is category saturation at the enterprise level, compressing what typically takes a decade of healthcare technology cycles into 36 months.
And yet, 20.9% of physicians still spend more than eight hours per week on the EHR outside normal work hours. That number has not moved since 2022.
📊 Despite ambient AI cutting note composition time by 15 percent or more, the "pajama time" metric that has defined physician overload since the EHR era has not moved in four years.
Ambient AI cleans the note. It does not clean the inbox. After the note comes 77 EHR inbox messages per day waiting for a primary care physician. The 14-step prior authorization that starts the moment the note is signed. The schedule compressed to 15-minute slots to hit RVU targets. Forty-seven percent of clinical time spent on tasks that are not direct patient care.
The best way to think about what ambient AI fixes: it recovers the time physicians spent transcribing, not the time they spend administering. Those are different categories of burden. And the administrative category is growing.
2. The Abridge Story and Why the Funding Makes Sense
Abridge was founded in Pittsburgh by Shiv Rao, a cardiologist at UPMC who built the early prototype because he wanted his own note-writing time back. The initial bet was simple: record the conversation, generate a structured note, integrate into the EHR. No new workflow. No new screen. Just less charting.
The enterprise distribution strategy was the breakthrough. Rather than selling to individual physicians or small practices, Abridge went directly to health system CIOs and CMOs with a full integration story - Epic, Cerner, Oracle Health. UPMC was the first major deployment. Then Kaiser Permanente. Then Yale New Haven Health. By 2026, Abridge is live in more than 100 health systems.
That distribution model is what justified the valuation escalation. At $250 million Series D, Abridge was proving product-market fit. At $300 million Series E, it was building the infrastructure to be the ambient AI standard across Epic-heavy U.S. health systems. At $316 million Series E extension, it was signaling that the competitive window is closing and the category leader is pulling away.
Competitors are real. Microsoft's Nuance DAX, acquired for $19.7 billion, dominates the enterprise market through the Dragon customer base and M365 integration. Ambience Healthcare just closed a $243 million Series C to compete across 100+ ambulatory subspecialties, EDs, and inpatient specialties. Abridge's integration depth in Epic creates a structural advantage that is hard to replicate.
3. The Safety Problem the Industry Is Not Talking About Loudly Enough

Modern ambient AI scribes report 95% to 98% accuracy in medical speech recognition. Those numbers are real. They are also incomplete.
The hallucination rate - instances where the AI adds clinical detail that was never spoken during the encounter - runs approximately 7% in some studies, though leading vendors cite 1 to 3% for their current models. For a technology that writes the legal medical record, a 1 to 3% error rate across millions of encounters per week is not a rounding error. It is a patient safety surface.
The highest-risk area is the physical examination section. AI systems have documented entire physical exams - reflexes, breath sounds, abdominal exam findings - for encounters where no physical exam occurred or was discussed. The model fills in what it expects to be there.
Other documented error modes include omitted symptoms, misattributed statements (patient words documented as physician statements), incorrect negations ("no chest pain" documented when chest pain was discussed), and overconfident phrasing where uncertainty expressed verbally is rendered as certainty in the note.
No ambient AI vendor accepts clinical liability for the notes generated by their software. The signing physician assumes full legal responsibility - for a note they may not have written and may have only briefly reviewed.
In November 2025, a class action was filed in San Diego Superior Court alleging that a health system deployed an ambient AI tool without proper patient consent. The complaint cited California's all-party consent wiretapping statute (CIPA) and the Confidentiality of Medical Information Act (CMIA). The case has not been resolved. More will follow.
📊 Physical exam hallucination rates in ambient AI systems run as high as 7 percent - meaning the technology documents clinical findings that were never observed or discussed in the encounter.

4. Who Is Being Left Behind
The ambient AI adoption story is predominantly an enterprise story.
Nuance DAX requires M365 infrastructure. Abridge requires Epic at scale. Ambience requires health system-level IT capability and negotiating leverage. For large academic medical centers and integrated delivery networks, the business case closes easily. Documentation time savings of 60 to 90 minutes per physician per day translate directly into incremental visits, RVU gains, and measurable burnout reduction.
For FQHCs, the math looks different.
Community health centers run on an average operating margin of negative 2%, according to NACHC and HRSA 2024 data. AI scribe subscriptions typically run $200 to $500 per provider per month in standard market pricing. A 20-provider FQHC implementing a midrange ambient AI tool at $300 per provider per month is looking at $72,000 per year in incremental costs on an organization that may already be running a deficit.
Approximately 60% of community health centers cite cost as the primary barrier to AI adoption. For rural health centers, that number rises to 70%.
The irony is real. The physician shortage in FQHC settings is more acute than in academic medicine. Burnout-driven attrition at community health centers directly affects access for the 34 million patients they serve. The population that most needs the productivity gain from ambient AI is the one least financially positioned to access the tools delivering it.
There are green shoots. The NACHC-eClinicalWorks partnership aims to bring AI documentation capabilities into community health settings at reduced cost. Athenahealth has moved to bundle ambient AI into its existing customer contracts with no additional charge. Some vendors have created specific community health pricing at $150 to $250 per provider per month.
But the gap remains wide. Enterprise health systems deploy ambient AI at scale. FQHCs run pilots, wait for grant funding, or go without.
5. The Governance Gap That No One Is Solving
Ambient AI has outpaced policy.
There are no federal standards governing ambient AI clinical documentation. There is no required accuracy threshold for AI-generated medical notes. There is no mandated disclosure framework for patients whose encounters are being recorded and transcribed by a third-party AI system. There is no liability framework that apportions risk between the AI vendor, the deploying health system, and the signing physician.
The ONC Interoperability Rule and the 21st Century Cures Act address data access and exchange, not note generation. The FDA, which regulates some clinical AI as a medical device, has not issued guidance specific to ambient documentation tools. The AMA has published ethical guidance but it carries no regulatory weight.
The November 2025 class action in California is the first but not the last legal challenge the industry will face. As ambient AI tools move from pilot to standard of care, the liability surface expands proportionally.
Health systems deploying ambient AI in 2026 are operating in a governance vacuum. Most have internal policies. Few have tested them in court. The physicians signing notes generated by ambient AI tools need to understand that their signature carries the same legal weight as a note they wrote themselves.
Deep Dive: The Ambient AI Business Case Across Four Provider Types
The investment thesis in ambient AI documentation is not uniform. It plays out differently depending on the clinical setting, payer mix, and technology infrastructure.
Large Academic Medical Centers
These are the early enterprise adopters. A 500-bed academic medical center with 800 physicians implementing Abridge at $300 per provider per month spends $2.88 million per year. If each physician captures 2 additional patient visits per day due to time savings, and average revenue per visit is $150, the annual upside is $87.6 million. The ROI closes quickly.
Beyond revenue, the soft benefits are measurable. A 21% reduction in burnout-related attrition in a physician workforce that costs $500,000 to $1 million per physician to replace translates into 7 to 10 figures of avoided replacement cost per year at scale.
Specialty Practices - Radiology and Pulmonology
Ambient AI is slower to penetrate procedure-heavy specialties. Radiology report generation already uses structured speech recognition via Dragon Medical. Adding a conversational layer for pre-read consultations and follow-up dictation is logical but requires specialty-tuned models. The hallucination risk in procedural documentation is higher - a misrecorded finding in a radiology report carries immediate clinical consequence.
For pulmonologists running lung cancer screening programs, the opportunity is in patient navigation notes and shared decision-making documentation, where time savings are significant and documentation complexity is high. CPT 0721T billing requirements mandate specific documentation of AI risk score review - ambient tools that can structure that documentation correctly reduce compliance burden meaningfully.
FQHCs and Safety-Net Clinics
The FQHC case is structurally different. These organizations carry the highest patient complexity, the lowest administrative capacity, and the tightest margins. The physician shortage is most acute here - more than 30% of FQHC clinical positions were unfilled in 2024. Burnout-driven attrition is the mechanism by which care access collapses.
The economic argument for deploying ambient AI at FQHCs is stronger than for any other provider type. The implementation capacity to execute it is weaker. Until bundled EHR pricing becomes standard and Section 330 grant guidance explicitly covers AI documentation tools as an allowable expense, the gap will persist.
What This Means For You
FQHC executives: Evaluate NACHC-eClinicalWorks partnership pricing and athenahealth bundled AI before signing any standalone scribe contract. The cost barrier is narrowing. Document any current AI scribe pilot with claims data - you will need the ROI evidence for the next grant cycle.
Health system CMOs: Ambient AI is now infrastructure, not innovation. If you are not deployed at scale, you are losing ground on physician satisfaction and recruitment. The Mass General Brigham 84-day data should be in your next board deck.
Radiologists and pulmonologists: Ambient tools designed for primary care do not automatically transfer to imaging or procedure specialties. Demand specialty-tuned model evidence and ask vendors for hallucination rates specific to your documentation type before signing.
Investors and founders: The enterprise distribution battle for ambient AI is largely won. Abridge and Nuance own the Epic/M365 world. The white space is in safety-net settings, specialty-specific documentation, and the governance layer - accuracy auditing, consent management, and liability allocation tools.
Policy advocates: The governance vacuum is real and actionable. The ONC, CMS, and state insurance commissioners all have existing regulatory authority that could reach ambient AI documentation practices. The November 2025 California class action provides the legal foundation for federal minimum consent standards.
Closing
Abridge's $5.3 billion valuation is not a story about hype. It is a story about a technology that genuinely works for the problem it was designed to solve, at a scale and speed that is rare in healthcare. The burnout data is real. The time savings are real. The enterprise adoption is real.
But the category is being built around the customers that can afford it. The providers that most need the burnout relief are the ones building the business case year by year on negative operating margins.
The most important question ambient AI investors and health system deployers should be asking in 2026 is not which vendor wins. It is who gets left behind when the category matures.
The technology has crossed the line from promising to proven. The governance frameworks have not followed. And the access gap between enterprise medicine and safety-net care is, as always, widening.
What are you deploying in your clinical environment? What is working and what is not? Reply to this email - I read every response.
About the Author
Jonathan Govette is the Co-Founder and CEO of Oatmeal Health, an AI lung cancer diagnostic company catching cancers earlier in the communities that need it most. Oatmeal uses AI to identify unscreened high-risk patients, navigate them to care, and score every lung CT for malignancy risk - billed under CPT 0721T. Stage I survival is 77%. Stage IV is 9%. We work in FQHCs because that gap is largest there.
Jonathan writes daily about radiology, pulmonology, AI diagnostics, health policy, hospital operations, and healthcare startups.
Subscribe to stay ahead of healthcare's most important shifts. Weekly deep-dives on AI, radiology, health policy, FQHCs, and the business of healthcare - written for operators, clinicians, and investors who want the signal, not the noise. Subscribe at oatmealhealthjonathangovette.substack.com
Key References
Abridge Series E funding ($300M, $5.3B valuation): MobiHealthNews / Technical.ly
Ambience Healthcare Series C ($243M): MobiHealthNews
Ambient AI market revenue ($600M, 2.4x YoY): 2026 Guide to Ambient Clinical Intelligence (Twofold)
Mass General Brigham 84-day burnout study (21.2% reduction): Becker's Hospital Review / Advisory.com
AMA 2025 National Physician Burnout Report (41.9%): Barton Associates
FQHC cost barrier (60-70%): FQHC Talent / NACHC 2025
Hallucination and safety data: IHS Online / MedCity News 2026
California class action (Nov 2025, CIPA/CMIA): MedCity News