

450K Lose Coverage: FQHCs Feel It First
450,000 New Yorkers lost health coverage on July 1. The uninsured wave is not a future risk for community health centers - it has already landed.

July 1, 2026. That date will appear in FQHC board minutes for years. It is the day 450,000 New Yorkers lost their health coverage - not due to a billing error, not due to a missed enrollment deadline, but due to a federal policy decision embedded in H.R. 1, the "One Big Beautiful Bill" signed into law in late June. The uninsured wave that health policy experts have been warning about for months is no longer a forecast. It has landed.

This is not primarily a story about insurance markets. It is a story about what happens to federally qualified health centers - the safety-net institutions built specifically to absorb coverage shocks - when the shock arrives faster, harder, and with fewer federal resources than at any point in the last two decades.

What Just Happened in New York
New York's Essential Plan was, until June 30, 2026, a model for how states could use ACA Section 1332 waiver authority to extend subsidized coverage to low-income residents. The Essential Plan provided $0-premium, $0-deductible coverage to residents earning between 138% and 250% of the federal poverty level - a population too income-high for Medicaid but historically priced out of the commercial market.
H.R. 1 eliminated federal matching payments for Essential Plan enrollees above 200% FPL effective July 1, 2026. New York faced a binary choice: absorb the cost entirely from state revenue, or end coverage for that income band. The state could not fill the gap in time. As a result, approximately 450,000 people - those earning between 200% and 250% FPL - lost their coverage on the first day of July.
The 1.3 million lower-income Essential Plan enrollees (below 200% FPL) retain their coverage under federal Medicaid matching. But the 450,000 who lost it face a replacement market with average premiums of $1,904 per month - up 114% from the $888 average in 2025, driven by the elimination of enhanced premium tax credits that H.R. 1 allowed to expire.
A family of three at 220% FPL - earning about $54,000/year - now faces monthly insurance premiums that exceed their rent. The math does not work. They will join the uninsured.
The National Picture Is Worse
New York's Essential Plan loss is dramatic because it happened all at once. But it is part of a broader, slower-moving collapse in coverage that has been building since 2025.
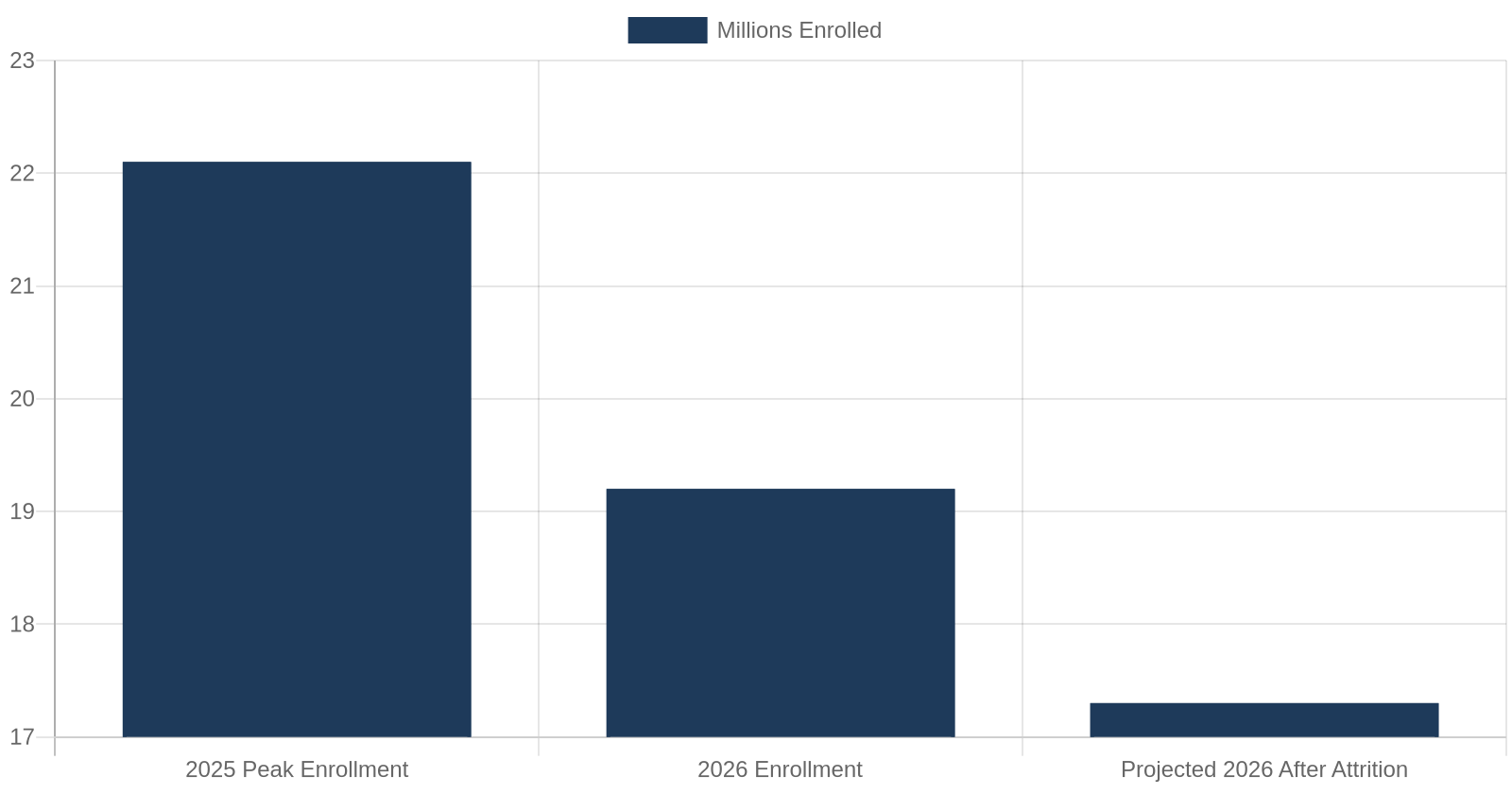
ACA exchange enrollment nationally fell from 22.1 million in 2025 to 19.2 million in 2026 - a decline of nearly 3 million people. The Congressional Budget Office projects that the reconciliation law's Medicaid cuts and premium credit rollback will produce 11.8 million more uninsured Americans by 2034. The Urban Institute estimates up to 7 million lose coverage by 2028 from work requirements alone.
The next major wave arrives January 1, 2027, when the Medicaid work requirement takes effect for expansion adults aged 19-64. CMS's own Interim Final Rule projects 2.3 million lose Medicaid in the first year, rising to 3.1 to 3.3 million in subsequent years. The CMS estimates are based on enrollment declines from administrative churn - people who are technically eligible but fail to document 80 hours of monthly qualifying activity. Of those projected to lose Medicaid, NACHC estimates 5.6 million are current health center patients.
FQHCs: The Institution Built for This Moment
Federally Qualified Health Centers exist precisely to serve patients regardless of ability to pay. They receive Section 330 federal grant funding, Medicare and Medicaid cost-based reimbursement, and are required by law to provide a sliding-scale fee schedule for uninsured patients. When coverage collapses, FQHCs are, by design, the place people go.
That design has a cost. And right now, that cost is accelerating past what many centers can sustain.

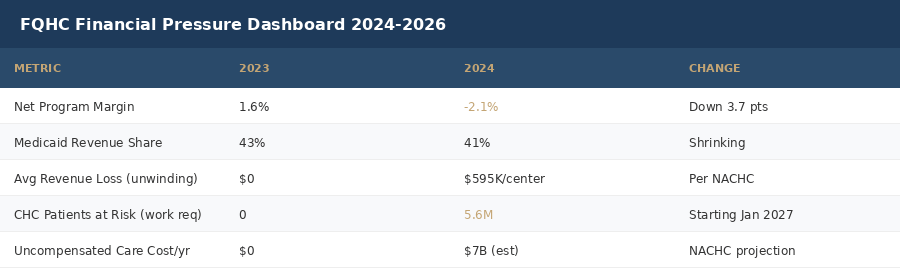
The numbers tell the story clearly. Health center net program margins averaged 1.6% in 2023 - thin but positive. By 2024, the sector had moved to a negative 2.1% margin, a 3.7 percentage point deterioration in a single year. The program posted a 2% loss in 2025. These are not individual centers struggling - this is a structural financial shift across the sector.
The proximate driver is the Medicaid unwinding that began in 2023 and has continued through 2025. The National Association of Community Health Centers reports that the average health center lost $595,000 in annual revenue from Medicaid unwinding alone - with large urban centers losing up to $20 million. The revenue loss is structural: patients who lose Medicaid don't disappear from the appointment schedule. They show up, receive care, and pay what they can on the sliding-scale fee - typically far less than the cost of service.
The $7 Billion Uncompensated Care Question
NACHC's projection is stark: $7 billion per year in additional uncompensated care costs for health centers if the coverage losses in H.R. 1 materialize as projected. To put that in context, the entire Section 330 federal grant program appropriation is approximately $7.4 billion annually.
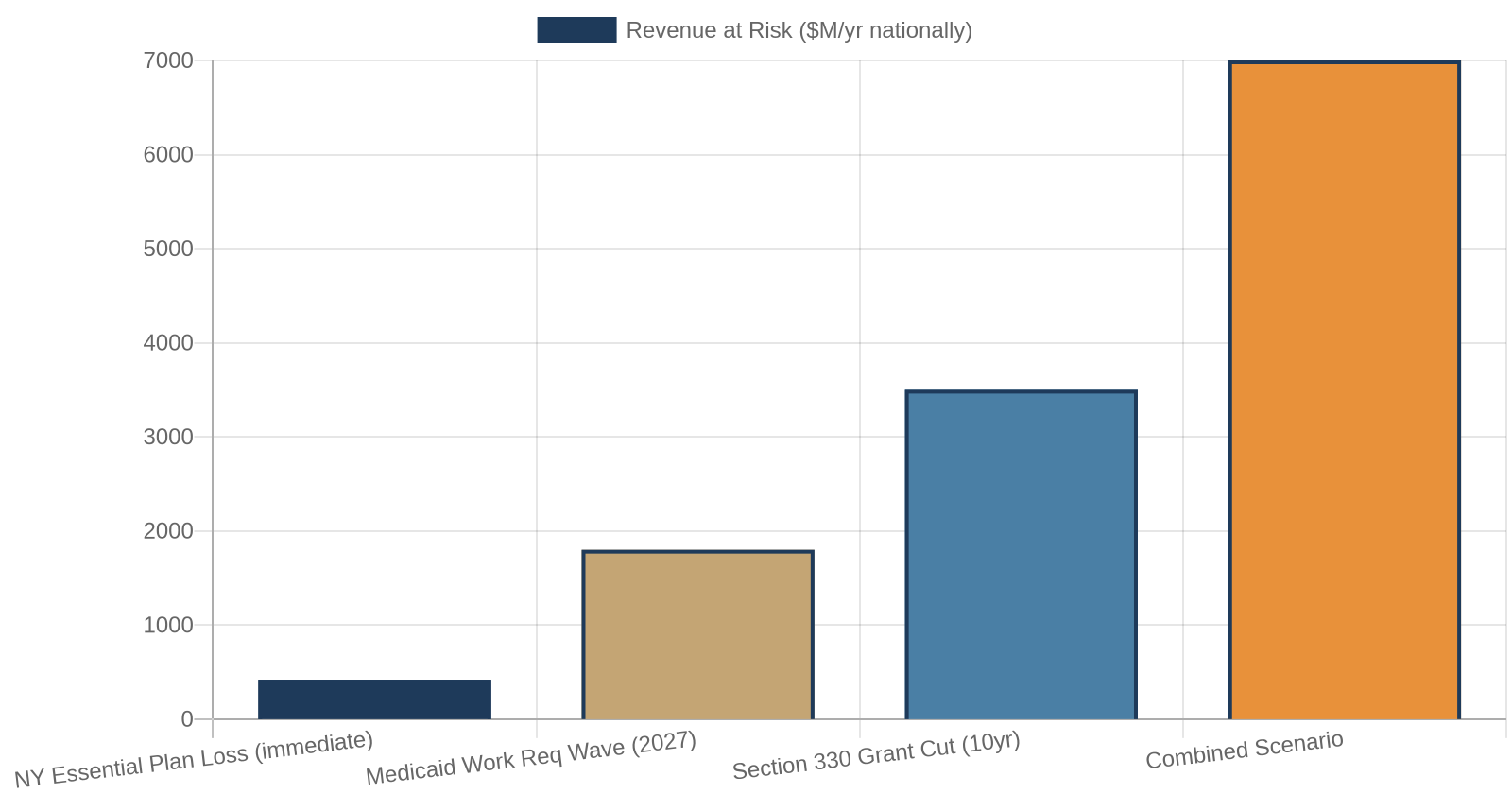
This means the coverage loss projected by CBO and the Urban Institute would create an uncompensated care burden approximately equal to FQHCs' entire federal operating grant. The math is unfeasible without either new federal investment, significant state subsidy, or service contraction.
Service contraction at health centers is not a hypothetical. It means reduced hours at rural sites. It means longer wait times at urban centers. It means behavioral health and dental services - historically the first to be cut - disappearing from the care model. It means the 31 million Americans who currently receive primary care at health centers finding that care harder to access, in the same moment that their insurance coverage has been stripped away.

The Work Requirement Timeline: What Comes Next
The immediate crisis - NY Essential Plan - is severe. But the structural pressure builds further in 2027. Here is the timeline that health center CFOs and policy teams are working against:
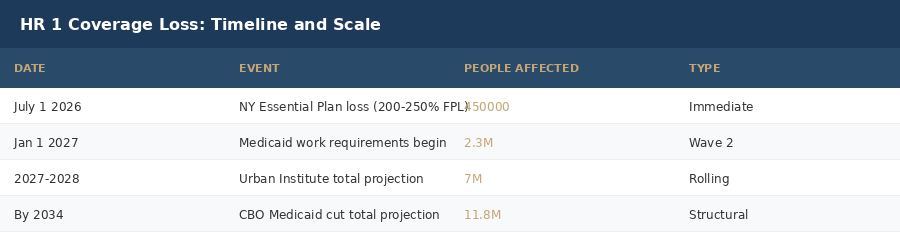
July 1, 2026: NY Essential Plan cut. 450,000 lose coverage immediately. Health centers in New York see uninsured volume rise.
October 2026: State Medicaid redetermination cycles accelerate under H.R. 1 requirements. Additional churn expected.
January 1, 2027: Federal Medicaid work requirement takes effect. 80 hours/month qualifying activity required for expansion adults 19-64. CMS projects 2.3M lose coverage in Year 1.
2027-2028: Urban Institute projects up to 7 million total coverage losses from work requirements. NACHC: 5.6 million of these are current health center patients.
By 2034: CBO projects 11.8 million more uninsured Americans from the combined effects of the reconciliation law.
Each milestone represents not just an insurance statistic but an operational event for health centers: more patients, more uncompensated care, more financial pressure, and - absent policy intervention - more service reduction.
Winners and Losers
Not everyone loses in this scenario. State budget offices that had been absorbing Medicaid expansion costs see reduced outlays, at least in the near term. Commercial insurers face a smaller Medicaid-enrolled population competing for exchange market share. The federal government reduces direct Medicaid outlays - which is the stated fiscal rationale for H.R. 1's coverage provisions.
The losers are more diffuse but more numerous: FQHCs and community health centers facing $7 billion in projected uncompensated care. Uninsured patients earning 200-250% FPL who now face $1,904/month premium options or go without. Rural health systems with no safety-net alternative when their local FQHCs contract. Emergency departments that will absorb the uninsured surge that community health centers can no longer buffer.
What Health Centers Are Doing Right Now

The health centers that are navigating this best are doing several things simultaneously. First, they are accelerating grant diversification - pursuing state innovation grants, HRSA pilot programs, and foundation funding to replace eroding Medicaid revenue. Second, they are implementing sliding-scale fee optimization, ensuring that uninsured patients are being enrolled at the highest fee tier the data supports rather than defaulting to the lowest. Third, they are investing in eligibility assistance staff - workers who can help patients navigate remaining coverage options, including Medicaid for those below 200% FPL and potential future state coverage programs.
Some centers are also engaging aggressively with state policy processes. New York, for example, has signaled interest in creating a state-funded replacement for the lost Essential Plan coverage, though no funded program has been announced. Health center advocacy organizations are pressing for emergency supplemental Section 330 grant funding to offset uncompensated care increases.
The political reality is that federal supplemental funding is unlikely in the current legislative environment. Centers that are waiting for a federal rescue are planning poorly. The centers that survive and continue to serve their communities will be those that are restructuring their financial models now - before the 2027 work requirement wave makes the current moment look manageable by comparison.
The Data Health Executives Should Be Tracking
For health system leaders and policymakers monitoring this situation, here are the metrics that matter most in the next 12 months:
Uninsured patient visit volume at FQHCs, tracked monthly. A sustained increase above 10% over 2024 baseline signals the financial inflection point is arriving.
Section 330 grant adequacy ratio: uncompensated care cost as a percentage of 330 grant revenue. Any ratio above 80% indicates a center operating at structural risk.
State Medicaid enrollment trends following H.R. 1 redetermination requirements. Month-over-month enrollment decline will indicate the pace of the coverage loss wave.
Emergency department utilization rates at hospitals in FQHC catchment areas. Rising ED visits for primary care-treatable conditions signal that the FQHC buffer is failing.
HRSA emergency grant applications and approval rates. A surge in emergency funding requests from centers will precede a wave of site closures or service reductions.
The Bottom Line
The 450,000 New Yorkers who lost coverage on July 1 are the first clear signal that the coverage architecture of the ACA era is being substantially dismantled. They are not the last. The January 2027 work requirement wave will be larger. The 2034 CBO projection will be reached through a series of smaller shocks, each one manageable-seeming in isolation, devastating in aggregate.
FQHCs were built to be the last line of health care access in America. That role is now being stress-tested at a scale and pace the system was not designed to handle. The centers that understand this, and are restructuring accordingly, have a chance to fulfill that mission through the next several years of policy turbulence. The ones waiting for the federal safety net to stabilize first may not survive long enough to find out what stabilization looks like.
The wave is not coming. It is here.
Sources: NACHC Federal Policy Report, June 2026; CBO H.R. 1 Coverage Effects Analysis, May 2026; Urban Institute Medicaid Work Requirements Impact Model, April 2026; CMS Medicaid Work Requirement IFR, Q2 2026; KFF Health Insurance Marketplace Report, 2026; New York Department of Health Essential Plan enrollment data; HRSA Health Center Program data, FY2024.